Pneumothorax causes, types, treatment, Who is at risk for pneumothorax?
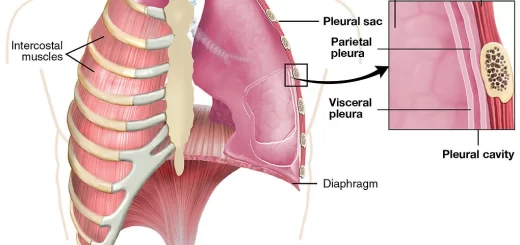
Pneumothorax is a medical condition in which air accumulates in the pleural space (the space between the lung and chest wall), causing the lung to collapse partially or completely. This can lead to breathing difficulties and, in severe cases, life-threatening complications.
Pneumothorax
Pneumothorax is the accumulation of air in the pleural space with a secondary collapse of the surrounding lung.
Types of Pneumothorax
• Pneumothoraces can be divided into spontaneous pneumothorax and traumatic pneumothorax.
- Spontaneous pneumothorax is sub-classified as either: Primary spontaneous pneumothorax or Secondary spontaneous pneumothorax.
- Traumatic (or nonspontaneous) pneumothorax occurs as accidental and as a result of blunt (non-penetrating) or penetrating trauma disrupting the lung, bronchus, or esophagus.
A subcategory of traumatic pneumothorax is iatrogenic pneumothorax, which occurs as a consequence of diagnostic or therapeutic maneuvers (i.e., thoracentesis, insertion of a central venous catheter, surgery, or mechanical ventilation).

Pneumothorax
Primary Spontaneous Pneumothorax
Primary spontaneous pneumothorax (PSP) is an entity that occurs most commonly in young men between the ages of 20 and 40 years of age. Although women have a much lower incidence of PSP, they tend to develop PSP 2 to 5 years earlier than men. A patient rarely presents with a primary episode after the age of 40 years.
Primary spontaneous pneumothorax occurs without a precipitating event in a person with no clinical evidence of lung disease. Many of these individuals have occult lung disease with subpleural blebs on computed tomography (CT) scans.
Secondary Spontaneous Pneumothorax
In contrast, secondary spontaneous pneumothorax occurs as a complication of underlying lung disease, most often chronic obstructive lung disease (COPD).
Etiology of Secondary Spontaneous Pneumothorax:
- Obstructive lung disease.
- Interstitial lung disease.
- Infection.
- Malignancy.
- Connective tissue disease.
Classification of pneumothorax according to the type of tear:
- Closed Type.
- Open Type.
- Tension Pneumothorax.
Clinical Picture
- Sudden stabbing chest pain.
- Exertional dyspnea.
- Dry cough.
- Tachypnea.
Clinical signs on examination
A. Inspection:
- Bulge in the affected hemithorax
- Limited respiratory movement
- Absent Litten’s sign
- Wider half of the subcostal angle.
B. Palpation:
- Limited chest expansion.
- Decreased TVF.
- Tracheal shift to the opposite side.
C. Percussion: Hyper-resonance
D. Auscultation:
- Decreased intensity of breath sound and VR.
- Bronchial breathing over collapsed lung.
- Amphoric breathing bronchopleural fistula.
In case of tension pneumothorax: Hypotension, shock, weak pulse, cyanosis.
Coin test (Coin sign): This sign is elicited by placing a large coin on the anterior chest wall and striking it with another coin, the observer listens over the back at a point directly opposite that the coin is struck. Normally a rather flat, clicking, poorly the sound is heard when the coin is struck over the front of the chest. When the test is carried out through a pneumothorax, the sound has a striking metallic, ringing quality due to the loss of the normal damping of the transmitted sound by the air-containing lung.
Investigations
Chest X-ray:
- Area of jet-black appearance devoid of lung reticulation found peripheral to a collapsed lung.
- Mediastinum shifted to the opposite side.
- May show hydropneumothorax or underlying lung disease.
Treatment (ICT drainage)
1. Observation
- Simple observation of the patient with a pneumothorax requires evidence that the air leak is sealed (i.e., that there is no further progression of the pneumothorax).
- This form of management is generally reserved for asymptomatic patients with a small (not greater than 20 percent) unilateral pneumothorax.
2. Aspiration
Some have advocated aspiration of a pneumothorax, with varied levels of success. These reports have prompted the British Thoracic Society to recommend simple aspiration as first-line therapy for all patients with first-time spontaneous pneumothorax.
This is in contrast to the American College of Chest Physicians Delphi Consensus Statement on this issue illustrating the controversial nature of this form of therapy.
The procedure consists of the insertion of a 16- or 18- gauge plastic catheters under local anesthesia using a sterile technique.
The recommended point of insertion is the second anterior intercostal space in the midclavicular line. The catheter is connected to a three-way stopcock and a large-volume syringe. Aspiration is performed until no further gas can be withdrawn. Follow-up chest radiographs are performed.
3. Tension Pneumothorax: Urgent insertion of wide pore needle, then ICT underwater seal.
4. Oxygen Inhalation.
5. Recurrent Pneumothorax. Intercostal tube insertion, pleurodesis or surgery
6. Bronchopleural Fistula. Surgery
7. Video-assisted thoracoscopic surgery (VATS) indicated in:
- Second ipsilateral pneumothorax.
- First contralateral pneumothorax.
- Synchronous bilateral spontaneous pneumothorax.
- Persistent air leak despite 5-7 days of chest tube drainage.
- Failure of lung re-expansion
- Professions at risk (e.g. pilots, divers).
You can subscribe to Science Online on YouTube from this link: Science Online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Pleural disease symptoms and treatment, What is the most common pleural disease?
Bronchiectasis causes, Is a bronchiectasis serious?, What is the best medication for bronchiectasis?
Suppurative Lung Diseases, Stages of Lung Abscess, Does a lung abscess require surgery?
Tuberculosis symptoms, What causes TB disease? and Can TB be transmitted through saliva?
Inflammation of the lung parenchyma, What causes lung parenchyma?, Is lung parenchyma dangerous
Hospital-Acquired Pneumonia Symptoms and Treatment, What is the difference between HAP and VAP?
Pneumonia causes, types, treatment, Is pneumonia usually serious? and Is pneumonia contagious?
Chronic Obstructive Pulmonary Diseases Treatment, Types and Causes of COPD
Steps of Asthma Control, What is good control of asthma? and What is asthma management?
Spirometry uses, What is a normal spirometry level? and What is FEV1 in spirometry?
Lung structure, borders, Lobes, Fissures, and Broncho-pulmonary segments