What are genitourinary disorders?, Kidney anomalies, Renal Cyst and Malrotated Kidney
Genitourinary anomalies are birth defects that affect the urinary system (kidneys, ureters, and bladder) or the genital tract (reproductive organs). These anomalies can range from mild to severe and can affect one or both sides of the urinary or genital tract.
Genitourinary anomalies
There are many different types of genitourinary anomalies, but some of the most common include:
- Kidney anomalies: These can include absent or underdeveloped kidneys, blocked ureters, or kidneys that are fused together.
- Bladder anomalies: These can include an underdeveloped bladder, a bladder that is in the wrong position, or a bladder that leaks urine.
- Ureteral anomalies: These can include blocked ureters, ureters that are too narrow, or ureters that are in the wrong position.
- Genital anomalies: These can include undescended testicles in males, hypospadias (where the urinary opening is on the underside of the penis) in males, and vaginal atresia (where the vagina is blocked) in females.
Genitourinary anomalies can be caused by a variety of factors, including genetics, environmental factors, and problems during pregnancy. The exact cause of most genitourinary anomalies is unknown. The symptoms of a genitourinary anomaly can vary depending on the type and severity of the anomaly. Some common symptoms include:
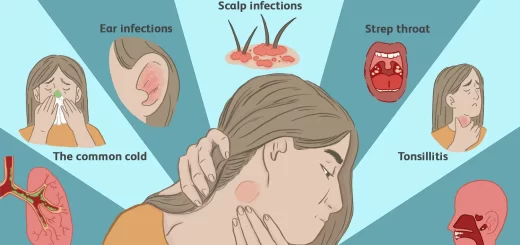
- Urinary tract infections (UTIs)
- Painful urination
- Difficulty urinating
- Blood in the urine
- Incontinence
- Frequent urination
- Abdominal pain
If you are concerned that your child may have a genitourinary anomaly, please see a doctor. Early diagnosis and treatment can help improve the outcome for children with genitourinary anomalies.

Anomalies of the kidney
Anomalies of the kidney
1. Renal Agenesis
Anatomical Consideration: At the level of the ureteric orifice, all muscle fibers in the walls of the ureter sweep towards the posterior wall (the anterior and lateral walls of the ureter become devoid of muscle and are lined by mucosa only). They continue into the trigone between the bladder mucosa and the detrusor by fanning out and join the muscle fibers from the opposite ureter.
Together they form the trigonal muscle that extends down to the bladder neck. The trigonal muscle is easily noted as an elevated layer in the trigone by cystoscopy. If one kidney is congenitally absent, its draining ureter and ureteric orifice are also congenitally absent. Consequently, the trigonal muscle on the same side will be absent, hence the term: hemitrigone.
- Congenital absence of one kidney in the presence of a normal contralateral kidney is a symptomless and harmless condition.
- It is discovered accidentally by imaging (ultrasound, IVU or CT scan) done for an unrelated complaint, or during cystoscopy which shows a hemitrigone with the absence of one ureteric orifice.
- The other kidney undergoes compensatory hypertrophy to maintain adequate renal function.
- A lifelong periodic urine analysis and renal ultrasound (at least once a year) should be done to detect and treat any pathological encounters that can jeopardize the contralateral solitary kidney.
- 5. Bilateral renal agenesis is rare and results in still born infants.
2. Anomalies in Size and Structure
Hypoplastic Kidney
- A small underdeveloped kidney is associated with a small undeveloped ureter and renal vessels.
- Even though the condition is urologically symptomless, reno-vascular hypertension can result from the associated renal artery stenosis and increased renin secretion to the circulation.
- Nephrectomy is indicated if reno-vascular hypertension develops.
Simple (Solitary) Renal Cyst
- It is usually unilateral and single. It is rarely bilateral and/or multiple.
- It is usually small but rarely reaches big sizes.
- It appears bulging from the kidney surface.
- It is covered by a very delicate epithelial wall and is filled with serous fluid (not urine).
- A small cyst is symptomless, harmless and requires no treatment.
- A big cyst (more than 10 cm in diameter) can cause bothersome dull aching renal pain.
- Diagnosis: IVU shows a space-occupying lesion (in the form of stretching of the calyx or splaying), e.g. cyst or renal cell carcinoma. Differentiation between both is possible by ultrasonography or CT scan.
- Surgical treatment is indicated only for large painful cysts. The kidney is exposed either surgically or laparoscopically. The roof of the cyst bulging from the kidney surface is completely excised with drainage of its content of serous fluid.
Polycystic Kidneys
Etiology
Congenital failure of fusion between the secretory system and excretory system. Glomerular secretion collects in the obstructed uriniferous tubules, turning them into cysts.
Types
(1) Adult type (most common):
- It affects 1 in every 1,000 births.
- It is autosomal dominant. It commonly runs in families from one generation to another.
- It is more common in females.
- Being a very slowly progressive disease, the clinical manifestations start to appear in the thirties or forties, hence the term “adult polycystic kidneys”.
- It is always bilateral. However, affection can be more advanced on one side than the other.
(2) Infantile type:
- Rare condition (1 in 10,000 births).
- Autosomal recessive.
- It is rapidly progressive and causes early childhood death.
Pathology
- The renal tissue is filled with: a huge number of small cysts; and peritubular fibrosis.
- The cysts contain clear serous fluid (not urine).
- In the advanced stage, both kidneys are hugely enlarged, with the destruction of the glomeruli from compression by surrounding cysts and peritubular fibrosis.
Clinical Picture
I. Adult type:
- Asymptomatic.
- Renal swelling: Usually bilateral, firm in consistency from the diffuse peritubular fibrosis and with a bossing surface.
- Renal pain occurs if secondary infection in the cysts.
- Total hematuria if a vessel in the wall of a cyst ruptures into a calyx or renal pelvis.
- Complications: Hypertension, osteomalecia, and renal impairment.
- In the late stages: manifestations of uremia (anorexia, nausea, vomiting, drowsiness, sense of fatigue, and anemia).
II. Infantile type:
- Oligohydramnios which affect the fetus‘s organ development.
- Intrauterine death due to pulmonary hypoplasia causing respiratory failure.
- Obstructed labor due to belly abdomen (enlarged kidneys).
- After labor death may occur due to respiratory failure.
- Rickets.
- Hypertension.
Investigations
- Laboratory studies: a. Early: normal blood tests. b. Late: renal Insufficiency in the form of proteinuria and specific gravity of a fasting urine sample +↑ serum creatinine, blood urea nitrogen, and potassium.
- Ultrasonography: diffuse small echo-lucent cysts filling both kidneys.
- Non-contrast CT abdomen and pelvis.
- MRU: both kidneys are replaced by cysts.
Complications
- Hypertension and renal insufficiency.
- Abdominal distension, GIT problems.
- Rickets and osteomalacia.
Treatment
- Conservative measures: ↓ protein diet, salts,↑ fluid intake, physical activity, manage hypertension, hypocalcemia, and infection.
- Hemodialysis or renal transplantation for end-stage renal disease.
- Nephrectomy if there is life-threatening hematuria or uncontrolled hypertension.
3. Malrotated Kidney
Normal Embryology
- In a 6-week-old embryo, both kidneys are present in the pelvis at the level of the sacral vertebra close to the midline, with each renal pelvis facing anteriorly.
- Both kidneys gradually ascend upwards and laterally and rotate medially.
- At full term, both kidneys reach the level of the upper 3 lumbar vertebrae further away from the midline, with each renal pelvis facing medially.
Etiology
Malrotation (failure of medial rotation) occurs:
- in the ectopic kidney;
- in horseshoe kidney;
- if there is failure of medial rotation despite normal ascent (rare).
Diagnosis by Intravenous Urography
- The renal pelvis and proximal ureter appear lateral to the lower calyx.
- The direction of the lower calyx is downward and medially instead of downward and laterally.
Clinical Picture and Treatment
The condition is symptomless, harmless, and requires no treatment.
4. Renal Ectopia
Simple Renal Ectopia
- An ectopic kidney that did not cross the midline. The commonest form is the pelvic kidney.
- A pelvic kidney can be palpated in the iliac fossa; its ureter is short and its blood supply is from the iliac vessels (not the aorta and inferior vena cava).
- The simple ectopic kidney is always malrotated.
- There are no symptoms, no complications, and no need for any form of treatment.
Crossed Renal Ectopia
- Rare condition.
- One kidney crosses the midline during intrauterine ascent. Both kidneys are on one side.
- The ureteric orifice of the crossed ectopic kidney is in its normal position.
- Both kidneys are separate or fused. This can be clarified by ultrasound or CT scan (not by IVU).
- The crossed ectopic kidney is always malrotated.
- If there are no symptoms or complications, so no need for any form of treatment.
Horseshoe Kidney
1. Horseshoe kidney is the commonest form of renal fusion where both lower poles are connected by an isthmus.
2. The ascent of the horse-shoe kidney during intrauterine life cannot proceed above the level where the isthmus reaches the inferior mesenteric artery at its origin from the aorta.
3. The isthmus, attached to both lower poles, prevents kidney rotation.
4. Intravenous urography shows:
- Lower position of both kidneys.
- Bilateral malrotation of the kidneys (the lower calyces are medial to the ureter and the pelvis is directed anteriorly).
- The longitudinal axis of the kidneys is directed downwards and medially (instead of downwards and lateral).
- Ureters lie on the body of vertebrae (instead normally lie on the transverse processes).
5. It is not treated unless it is associated with a pathology e.g. stones, tumor, pelvi-ureteric junction obstruction.
You can subscribe to Science Online on Youtube from this link: Science Online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Functions of Kidneys, Role of Kidney in glucose homeostasis, Lipid & protein metabolism
Urinary system structure, function, anatomy, organs, Blood supply & Importance of renal fascia
Suprarenal glands (adrenal glands) anatomy, structure & Effect of Deficiency of Catecholamines
Histological structure of kidneys, Uriniferous tubules & Types of nephrons
Urine formation, Factors affecting Glomerular filtration rate, Tubular reabsorption & secretion
Functions of the loop of Henle, distal tubules, collecting ducts & Glucose tubular maximum