Importance & types of fungi, Opportunistic infections and Predisposing factors to candidosis
Medical mycology is the study of mycoses of man which are the diseases caused by fungi. Of thousands of species of fungi known, less than 100 are pathogenic to man. Fungi are widespread in nature, the natural habitat for most species being the soil.
Medical importance of fungi
- Antibiotics. Substances produced by fungi that are used as antibacterial therapeutic agents, e.g. penicillin.
- Ergot: fungal product with profound toxic characteristics, which at proper dosage levels has long held an important place in pharmacology e.g. inducing uterine contractions and controlling bleeding, treating migraine.
- Toxins: The most generally recognized toxic genus is Amanita, or toxic mushroom, These fungi induce intoxication and hallucination. Aspergillus flavus produces a powerful toxin, aflatoxin, which is generally (incriminated in liver malignancy i.e. Hepatoma.
- Mycoses: Mycoses are fungal diseases that affect the human body. They are classified according to the affected body site (Topographically) into:
I. Superficial mycoses: These are caused by fungi that affect the superficial layers of the skin (epidermis and dermis) e.g: Dermatophytosis, Pityriasis Versicolor, Piedra, and Tinea Negra.
II. Subcutaneous mycoses: These are caused by fungi that affect the subcutaneous layers e. g.: Mycetoma, Chromomycosis, and Sporotrichosis.

Differences between Bacteria and Fungi
III. Systemic mycoses:
- Pathogenic mycoses e.g. Histoplamsosis.
- Opportunistic mycoses: Aspergillosis, Candidosis, Pneumocystis jiroveci infection, Cryptococcosis, and Mucormycosis.
Classification and Morphology
Fungal Cell Wall: The fungal cell wall is composed of a complex network of proteins and polycarbohydrates that varies in composition depending on the fungal species.
Fungal Cell Membrane: Sterols account for approximately 25% of the weight of the cell membrane, Whereas mammalian cell membranes contain primarily cholesterol, ergosterol is the predominant sterol in many pathogenic fungi.
Differences between Bacteria and Fungi
- Fungi are eukaryotes (the fungal cell has a membrane-bound nucleus) while bacteria are prokaryotes.
- Bacteria are single-celled whereas most fungi are multicellular except for yeast.
- Different compositions of the cell walls. The cell wall of bacteria is composed of peptidoglycan, whereas fungi cell walls are made up of chitin which is a nitrogen-containing polysaccharides.
- Fungi are heterotrophs while bacteria can be autotrophs or heterotrophs.
- Bacteria have shapes different from fungi.
- Bacteria reproduce asexually via binary fission whereas fungi are capable of reproducing both asexually (production of spores, budding, fragmentation) or sexually (production of zygotes).
- The fungal cell has organelles such as endoplasmic reticulum, Golgi bodies, ribosomes, vacuoles, and mitochondria.
Morphological classification
According to microscopic morphology, fungi are divided into four groups:
- Filamentous fungi (molds): These fungi occur in the form of long branching filaments or true hyphae, which intertwine to produce a mass of filaments or mycelium. E.g.: Aspergillus, dermatophytes
- Yeasts: These occur in the form of round or oval bodies which reproduce by the formation of buds known as blastospores, The only pathogenic yeast in medical mycology is Cryptococcus neoformans.
- Yeast-like fungi: These are fungi that occur in the form of budding yeast-like cells and as chains of elongated unbranched filamentous cells which resemble the appearance of true hyphae pseudohyphae), These pseudohyphae intertwine to form a pseudomycelium, The yeast-like fungi are grouped together in the genus Candida.
- Dimorphic fungi: These are fungi that exhibit a filamentous mycelial morphology (the saprophytic phase) when grown at room temperature but have a typical yeast morphology (parasitic phase) inside the body and when grown at 37°C in the laboratory (e.g histoplasmosis).
Opportunistic infections
Aspergillosis
These are fungal diseases due to a group of fungi of the genus Aspergillus. These saprophytic fungi are pathogenic only under certain conditions of immunosuppression. The disease is usually sporadic in distribution. The clinical picture is dominated mainly by respiratory manifestations.
Causative Agents
A. fumigatos, causes 90% of diseases.
Clinical presentation
Pulmonary Aspergillosis: This can be further subdivided into:
1. Aspergilloma
This is the most frequent form of aspergillosis, represent about 85% of all cases of aspergillosis. It is defined as the development in situ of Aspergillus in a pre-existing lung cavity. Usually on the apex of the lung. The disease is rarely bilateral and sometimes multiple. The pre-existing cavity is usually a healed tuberculous cavity. Other cavities include bronchiectasis, emphysema, carcinoma, congenital cysts…etc. Males are more affected than females. The disease is rare below the age of 12 years. Clinical diagnosis depends upon the triad of Deve:
- Recurrent hemoptysis.
- Typical X-ray pictures.
- Absence of acid-fast bacilli in sputum.
Laboratory diagnosis
Specímen: sputum
Detection of Aspergillus in sputum either by direct microscopic examination using KOH preparations or by culture on Sabouraud’s Dextrose agar incubated at 37- 40° C, which reveals green colonies with a central dome of the conidiophore. Aspergillus appears as filamentous septate structures that usually branch.
The conidiophores carry characteristic radiating chains of conidia spores, Demonstration precipitating antibodies (by double diffusion methods) in the patient’s serum. Histopathological examination of lung biopsy possible.
2. Allergic bronchopulmonary aspergillosis: (ABPA)
This disease affects mainly atopic subjects presenting with bronchial asthma and labile pulmonary infiltrate, There is also high eosinophilia in the peripheral blood and in the sputum, Precipitins are present only in 60 % of cases.
Candidosis
Candida is common in the microflora of the atmosphere. C Albicans (the most frequent etiologic agent) are present in the mucous membranes of the alimentary tract and vagina in 10-50% of healthy subjects. It is never present as a saprophyte in blood or other internal fluid or in the tissues.
Predisposing factors to candidosis
1- Physiological:
- Pregnancy.
- Infancy and old age.
- Obesity.
2- Pathological:
- Neoplasms (especially leukemia and Hodgkin’s disease).
- Endocrinopathy (especially diabetes mellitus).
- Autoimmune disease (Chronic mucocutáneous candidosis).
- Debilitation.
- Drugs: Antibiotics, Cytotoxic drugs, Corticosteroids, Oral contraceptives.
- Surgery: Renal transplantation.
- Radiotherapy.
- Peritoneal dialysis.
Clinical manifestations
1. Gastrointestinal Candidosis
- Oral Candidosis (thrush): Oral thrush is seen most commonly in the newborn, it is also seen in diabetic patients and debilitated aged patients and in those receiving intensive antibiotics or corticosteroid therapy.
- Enteric Candidosis: The disease is rarely suspected and even less commonly diagnosed ante-mortum, However, Candida has been shown to be the etiologic agent of cases of diarrhea that have subsided after treatment with the antifungal drug.
2. Candida intertrigo
Occurs due to exposure to heat and humidity and to topical moisture as in bedridden compromised patients.
3. Onychia and Paronychia
Candidosis of the nail bed is a chronic condition often associated with the frequent immersion of hands in water.
4. Vaginal and Vulvo-vaginal Candidosis
The disease is common during pregnancy and in diabetic patients.
5. Bronchial and pulmonary Candidosis
Patients with chronic bronchial disease or pulmonary infection treated with antibiotics have increased Candida counts in their sputum.
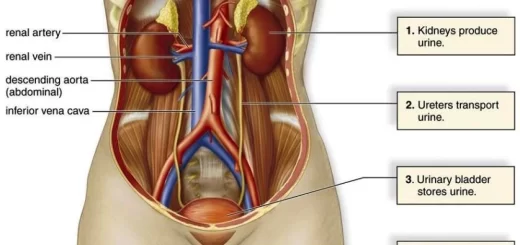
6. Renal Candidosis
Candiduria may indicate either benign colonization or true infection of the urinary tract, Candida can cause pyelonephritis and cortical renal infection.
7. Candida septicaemia
It occurs only in severely compromised patients.
You can follow science online on YouTube from this link: Science online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Life cycle of varicella zoster virus, Cytomegalovirus & Diagnosis of Infectious mononucleosis
Vaccines types, Live vaccines, Inactivated vaccines, Subunit vaccines, Naked DNA & mRNA vaccines
Adaptive (Acquired immunity) types, Difference between Innate & Adaptive Immune responses
Features and classification of viruses, Defective viruses & Viral vectors used for gene therapy
Cytokines function, use, definition, inflammation & side effects