Intestinal Obstruction causes, types, What are 3 signs of intestinal obstruction?
Intestinal obstruction occurs when there is a blockage in the intestines that prevents food, fluids, and gas from passing through normally. This can happen in the small intestine or the large intestine (colon) and can be partial or complete.
Intestinal Obstruction
The luminal contents cannot pass through the gut tube.
Epidemiology:
- 1% of all hospitalizations.
- 3% of emergency surgical admissions.
- Mortality rate: 3% for simple bowel obstruction, 30% when there is strangulation or perforation.
Intestinal obstruction has several types and can be classified in several ways:

Intestinal Obstruction
Duration:
- Acute obstruction: Small bowel obstruction (SBO).
- Chronic obstruction: Large bowel obstruction (LBO).
- Acute-on-top of chronic: obstruction starts as large-bowel and progress as small-bowel due to yielding of ileo-cecal valve.
Extent: Partial or Complete.
Interference with blood supply:
- simple bowel obstruction: Occluded lumen without interference with blood supply.
- Strangulated bowel obstruction: Occluded lumen with interference with blood supply.
Etiology:
1. Mechanical (Dynamic) Obstruction: peristalsis working against obstructing agent trying to overcome it (this peristalsis is always heard by auscultation & could be seen on inspecting the abdomen as a wave-like movement).
Causes of mechanical obstruction
- Intraluminal: e.g. impacted faces (in (rectum) mainly). (bezoars) (partially digested or undigested material). gallstone (in elderly, 2ry to erosion of large gallstone through GB into duodenum & classically, there is impaction 60 cm proximal to ileo-cecal valve). and Ascaris lumbricoids.
- Intramural: e.g. malignant (e.g. colon cancer), inflammatory stricture (e.g. IBD), radiation stricture, post-ischemic stricture.
- Extramural: e.g. bands/adhesions, hernias, volvulus, intussusception or carcinomatosis.
2. functional (dynamic) Obstruction: luminal contents cannot pass through the gut tube because of disturbances in gut motility that prevent coordinated peristalsis from one region of the gut to the next i.e. absent mechanical element.
Causes of functional obstruction:
1. Vascular occlusion ileus,
2. Adynamic or inhibition (no peristalsis): e.g.(paralytic ileus):
- Post operative.
- Metabolic causes: (DKA), hyponateremia, hypokalemia or hypomagnesaemia.
- Drugs: morphine, TCA, antacid or anticonvulsant.
- Intra-abdominal inflammation, sepsis, or occult wound infection.
- Pneumonia, renal stone, retroperitoneal hematoma or fracture of the spine and ribs.
3. Spastic ileus (intestine remains contracted and not propulsive) c.g.
- mesenteric vascular occlusion [MVO], or pseudo-obstruction.
- Uremia, Porphyria, Heavy metal poison.
Proximal to the site of obstruction:
1. Stage of Hyperperistaltic with anti-peristaltic waves: occurs early in the trial to overcome the obstruction.
2. Stage of dilatation (due to exhaustion and paralysis).
The loop becomes distended with:
- Fluids: swallowed, secreted & diffused from blood. The secreted part alone is more than liters per day (Saliva: 1-1,5L, gastric juice: 1,5-2,5L, bile: IL, pancreatic secretion: 1,5L, intestinal secretion: 3L).
- Gases: either swallowed (70%), diffused from blood (20%) or produced from putrefaction of food (10%).
3. Late: bacterial proliferation with the breakdown of retained intestinal contents produces. toxins that accumulate in the stagnant fluid and do not pass to the circulation except after the release of obstruction, which may lead to toxemia which may be fatal.
Distal to obstruction:
- Early normal peristalsis to evacuate the residual contents.
- Late: the distal segment is empty, collapsed, contracted, and immobile.
At the site of obstruction:
- Simple obstruction: the strangulated loop becomes distended with gas & fluid.
- Strangulated obstruction:
- At first, the venous flow is occluded (being of low pressure) leading to edema and congestion.
- Arterial flow is then occluded leading to Ischemia and gangrene.
- The devitalized wall of the Intestine permits the passage of toxins & bacteria to the peritoneal cavity & circulation causing toxemia.
- Lastly, perforation leads to peritonitis.
Strangulation may be due to:
- External compression; hernial orifices/ adhesions/bands.
- Interruption of mesenteric flow: Volvulus or intussusception.
- ↑ intra-luminal pressure: closed-loop obstruction. (bowel is obstructed at both, proximal & distal points e.g. volvulus and tight carcinomatous stricture of the colon with a competent ileo-cecal valve).
- Iry obstruction of intestinal circulation: mesenteric infarction.
Clinical picture:
The four cardinal symptoms of bowel obstruction:
- Pain: Colicky abdominal pain.
- Vomiting and Nausea.
- Abdominal distension.
- Absolute constipation: Passage of flatus and/or stool up to 6 hours after presentation may occur and does not exclude intestinal obstruction.
These features vary according to:
- Location of the obstruction:
- Duration of the obstruction
- Presence or absence of intestinal ischemia: strangulated obstruction with ischemia → tachycardia, localized abdominal tenderness, fever, marked leukocytosis, acidosis.
- Underlying pathology:
- Intra-abdominal adhesions related to prior abdominal surgery are the most common etiologic factor of small bowel obstruction.
- In contrast to colonic obstruction, SBO is uncommonly caused by neoplasm.
- cancer-related SBO is more commonly caused by extrinsic compression or invasion by advanced malignancies arising in organs other than the small bowel.
- Superior mesenteric artery (SMA) syndrome; a rare etiology of obstruction caused by compression of the 3rd part of duodenum by the SMA as it crosses over it.
Complications:
- Hypovolemic shock: due to fluid loss by vomiting, sequestration of fluids in the third space (dilated loops). In strangulated obstruction: shock is more marked due to additional blood loss into the strangulated loop.
- Dehydration and electrolytes imbalance: hyponatraemia & hypokalemia.
- Toxemia: in strangulated obstruction.
- Perforation & peritonitis.
According to LAPLACE’S law: maximum pressure is at the maximum diameter area. So-Caecum is at the greatest risk of perforation.
Diagnosis:
The Strategy of Diagnosis: the aim of work-up for diagnosis is to:
- Distinguish mechanical obstruction from ileus
- Determine the etiology of the obstruction
- Discriminate partial from complete obstruction.
- Discriminate simple from strangulating obstruction.
Tools of Diagnosis:
1. History and physical examination
Four cardinal symptoms: Pain (Location and characteristic of pain), Vomiting, distension and constipation.
Examination:
general examination: Vital signs. (PR-Temp-BP) and Hydration status.
Abdominal and rectal examinations:
- INSPECTION: Abdominal distention, scars-visible peristalsis.
- PALPATION: Mass, tenderness, guarding & Examination of hernial orifices.
- PERCUSSION: Tympanic, dullness.
- AUSCULTATION: Bowel sounds are high pitch and increase in frequency or silent.
2. Laboratory investigations:
- CBC: increase Hematocrit (dehydration) and increase in WBC.
- KFT (kidney function test): increase in BUN (blood urea) and creatinine. lactic dehydrogenase useful but not sensitive to rule out necrosis.
- Arterial blood gases (ABG): metabolic alkalosis and respiratory acidosis.
3. radiology:
X-ray:
1. Abdominal X-ray:
Small bowel obstruction: triad of:
- dilated small bowel loops 3 cm in diameter.
- air-fluid levels that are generally central a lie transversally in a step-ladder fashion.
- no air in the colon.
site: Jejunum (valvulae conniventes) or ileum (featureless).
Large bowel obstruction: triad of:
- dilated large bowel loops (proximal colon > 9 cm & sigmoid colon > 5cmy in diameter).
- peripheral distention with haustral folds which, unlike valvulae conniventes, are spaced irregularly & indentations are not placed opposite one another.
- They do not usually traverse the complete width of the bowel.
- site: Cecum (rounded gas shadow in the right iliac fossa).
The cause of bowel obstruction can often determined:
- Presence of pneumobilia, suggest G.S ileus.
- pathognomnic images of Sigmoid volvulus (coffee beans sign) and cecal volvulus.
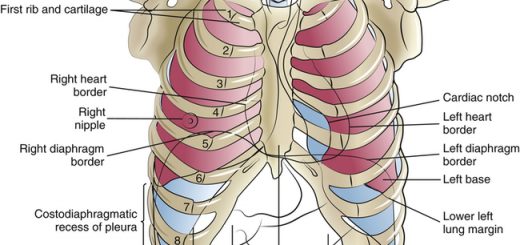
2. chest X-ray:
- Detect extra-abdominal conditions present with bowel obstruction e.g. fracture rib & pneumonia.
- The presence of pneumoperitoneum indicates perforated viscus.
Contrast studies:
Uses: Indications are controversial.
- Identify the site and often the cause of obstruction.
- Differentiate between colonic and distal small bowel obstruction.
- Differentiate between ileus-partial and complete obstruction.
Barium should not be used in a patient with peritonitis
CT scans (most important):
- Recently become valuable in B.O. especially when plain films failed in diagnosis or suspect strangulation.
- Accuracy 94%, Sensitivity 93%, and specificity 100% in the diagnosis of bowel obstruction.
treatment:
For optimal treatment to be instituted, five questions must be answered:
- Is the diagnosis intestinal obstruction?.
- Is the obstruction mechanical?.
- What is the level of obstruction?.
- Is there evidence of bowel wall ischemia or perforation?.
- How severe are the associated systemic disorders?
resuscitation and conservative treatment:
- NBO and gastric decompression using a nasogastric (NG) tube to reduce nausea, distension, and the risk of vomiting and aspiration.
- Fluid & electrolyte resuscitation.
- Urinary catheter insertion to calculate the urine output (UOP).
- Blood transfusion and/or blood products (FFP), if needed.
- Antibiotics as bacterial translocation may occur in the sitting of bowel obstruction.
- good observation of the patient: including the observation of vital signs, abdominal examination, and serial film of X-ray.
1. indications of conservative treatment:
- incomplete obstruction.
- if suspect adhesive intestinal obstruction (scar of previous abdominal surgery).
- advanced malignancy.
2. Surgical Treatment:
When to operate? Not too early and not too late.
Indications of surgical intervention:
- Obstructed or strangulated external hernia.
- Internal intestinal strangulation.
- closed loop obstruction.
- generalized or localized peritonitis.
- perforation
- failure of conservative treatment.
Aim of surgery? operate before the onset of irreversible ischemia
How to operate? What to do?
Operative assessment is directed to:
- The site and nature of obstruction.
- The viability of the gut: non-viable bowel is resected.
Criteria suggesting viability: normal color, peristalsis & marginal arterial pulsations
Exploration:
- Incision: Midline Right paramedian.
- Palpate the cecum: Distended cecum = LBO, while collapsed cecum = SBO.
- dealing with the cause.
- Adhesions→ Division (lysis).
- Bands→ Release (cut).
- Hernias→ Reduction & repair.
- Tumors → Resection or bypass or diverting stoma (ileostomy colostomy).
You can subscribe to Science Online on YouTube from this link: Science Online
Gastroesophageal Reflux Disease, Complications of GERD, and Barrett’s oesophagus
Esophagus diseases, Dysphagia causes, Achalasia, and Symptomatic Diffuse Esophageal spasm
Pharynx function, anatomy, location, muscles, structure, and Esophagus parts
Tongue function, anatomy, and structure, Types of lingual papillae, and Types of cells in taste bud
Mouth Cavity divisions, anatomy, function, muscles, Contents of Soft palate and Hard palate
Temporal and infratemporal fossae contents, Muscles of mastication and Otic ganglion