Gallbladder diseases, Types and risk factors of Gallstones, Parasites associated with cholelithiasis
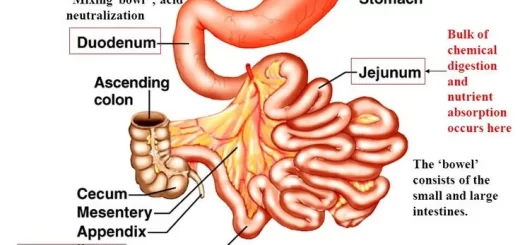
The gallbladder is a sac located under the liver, It stores and concentrates bile produced in the liver, Bile helps in the digestion of fat and is released from the gallbladder into the upper small intestine (duodenum) in response to food (especially fats), Gallstones are the most common biliary pathology.
Congenital GB diseases
- Double GB.
- Y cystic duct.
- Bilobed GB.
- Folded GB.
- Retroserosal.
- GB Diverticulum.
- Hourglass GB.
- Intrahepatic GB.
- GB with mesentery.
Gallstones
Epidemiology
Gallstones affect 10-20% of the adult population, Far more common in women, with a female ratio of approximately 2:1, People of advancing age (as compared to young aged), female sex with a tendency to obesity, and a history of rapid weight loss are particularly prone to develop cholesterol stones, Pigmented stones, on the other hand, are far more often seen in people, particularly with disorders of hemoglobin, resulting in an increase in hemolysis.
Prevalence of Gallstones in Egypt
- In Egypt 20%.
- Prevalence in women is twice that in men.
- Among cirrhotics 30%.
- Prevalence is higher among diabetics after gastrectomy, ileal resection with hypolipidemic drugs, long-term octreotide, and contraceptive pills.
Risk factors
- Female sex, obesity, increased age.
- American Indian ethnicity & Western diet.
- Positive family history.
- Certain drugs: pills, anabolic steroids, and hypolipidemic drugs.

Gallbladder diseases
Types of stones
- Cholesterol stones.
- Pigment Stones (brown/black).
- Mixed stones.
Parasites commonly associated with cholelithiasis
- Fascioliasis.
- Ascariasis
- Schistosomiasis.
- Clonorichiasis sinsesis (Precancerous) Found in far east, Precancerous to cholangiocarcinoma.
Pathophysiology
Biliary sludge (mud) is often a precursor of gallstones, It consists of Ca bilirubinate (a polymer of bilirubin), cholesterol microcrystals, and mucin, Sludge develops during gallbladder stasis, as occurs during pregnancy or while receiving TPN (total parenteral nutrition), Most sludge is asymptomatic and disappears when the primary condition resolves, Alternatively, sludge can evolve into gallstones or migrate into the biliary tract, obstructing the ducts and leading to biliary pain, cholangitis, or pancreatitis.
Nucleation
The excess cholesterol must precipitate from the solution as solid microcrystals, Such precipitation in the gallbladder is accelerated by mucin, a glycoprotein, or other proteins in bile, The microcrystals must aggregate and grow, This is facilitated by the binding effect of mucin forming a scaffold (nucleus) and retention in the gallbladder (impaired contractility from the excess cholesterol in bile), Once cholesterol crystals begin to agglomerate and form clusters the stones are inevitable (about 2mm /year).
Nucleating factors:
- Several specific heat labile glycoproteins.
- Gall bladder mucus.
- Biliary calcium.
- Alteration in gallbladder prostaglandin metabolism.
- Gallbladder stasis.
- Altered gall bladder absorption.
Types of Gallstones
Gallstones grow at about 1 to 2 mm/year, taking 5 to 20 years before becoming large enough to cause problems, Most gallstones form within the gallbladder, but brown pigment stones form in the ducts, Gallstones may migrate to the bile duct after cholecystectomy or, particularly in the case of brown pigment stones, develop behind strictures because of stasis and infection.
1. Cholesterol stones
- 85% of gallstones especially in the Western world.
- For cholesterol gallstones to form, Bile must be supersaturated with cholesterol.
- Normally, water-insoluble cholesterol is made water-soluble by combining with bile salts and lecithin to form mixed micelles.
- Supersaturation of bile with cholesterol most commonly results from:
- Excessive cholesterol secretion (as occurs in obesity or diabetes).
- Decrease in bile salt secretion (e.g., in cystic fibrosis because of bile salt malabsorption).
- Decreases in lecithin secretion (e.g., in a rare genetic disorder causes a form of progressive intrahepatic familial cholestasis).
2. Pigment stones
- Black pigment: Stones are small hard gallstones composed of Ca bilirubinate and inorganic Ca salts (e.g., Ca carbonate, Ca phosphate). Factors that accelerate the development: Alcoholic liver disease, Chronic hemolysis, and Older age.
- Brown pigment: Stones are soft and greasy consisting of bilirubinate and fatty acids (Ca palmitate or stearate), They form during infection, inflammation, and parasitic infestation (e.g., liver flukes in Asia).
3. Mixed stones
Symptoms & Signs
About 80% are asymptomatic, The remainder have symptoms ranging from biliary-type pain (biliary colic) to cholecystitis to life-threatening cholangitis. (Ascending cholangitis), Nausea and sometimes vomiting are common, but fever and chills do not occur unless cholecystitis has developed, Mild right upper quadrant or epigastric tenderness may be present; peritoneal findings are absent, Between episodes, patients feel well, Biliary colic is the most common symptom.
- Gallstone migration, into the cystic duct which, even if transient, causes biliary colic.
- Characteristically begins in the right upper quadrant but may occur elsewhere in the upper abdomen.
- It is often poorly localized, particularly in diabetics and the elderly.
- The pain may radiate into the back or down the arm.
- Episodes begin to suddenly become intense within 15 min to 1 h, remain at a steady intensity for up to 12 h (usually < 6 h), and then gradually disappear over 30 to 90 min, leaving a dull ache.
- The pain is usually severe enough to send patients to the emergency department for relief.
Clinical findings
- Shallow respiration, fever.
- Jaundice.
- Murphy’s sign is positive (Tenderness with examination).
- Tender mass at GB region.
- WBC is high.
Biliary-type pain
- Although biliary-type pain can follow a heavy meal, fatty food is usually a precipitating factor.
- Nonspecific Gl symptoms, such as gas, bloating, and nausea, have been commonly associated with gallbladder disease.
- Little correlation exists between the severity and frequency of biliary pain and pathologic changes in the gallbladder.
- pain can occur in the absence of cholecystitis.
- Pain last > 12 h, particularly if accompanied by vomiting or fever acute cholecystitis or pancreatitis is likely.
Prognosis
Those with asymptomatic gallstones become symptomatic at a rate of about 2%/year, The symptom that develops most commonly is biliary pain rather than a significant biliary complication, Once biliary symptoms begin, they are likely to recur; Pain returns in 20 to 40% of patients/year, While about 1 to 2% of patients/year develop complications such as cholecystitis, choledocholithiasis, cholangitis, and gallstone pancreatitis.
You can subscribe to Science Online on YouTube from this link: Science Online
You can download the Science Online application on Google Play from this link: Science Online Apps on Google Play
Cholecystitis types, causes, symptoms, diagnosis, treatment, and complications of Gall stones
Vascular Liver Disorders, Causes and risk factors of Budd-Chiari syndrome
Autoimmune Hepatitis symptoms, types, diagnosis, causes and treatment
Primary biliary cirrhosis symptoms, cause, diagnosis, treatment, and Osteoporosis
Diagnosis of the cause of jaundice, Hepatobiliary imaging, treatment of cholestasis and Pruritus
Liver Cholestasis types, causes, features, symptoms, diagnosis, and treatment
Jaundice symptoms, types, cause, treatment and What is the source of bilirubin?
Liver failure, symptoms, stages, cause, treatment, Acute on chronic liver failure (ACLF)
Hepatic Artery Embolization, Importance & risks of Embolization therapy for Liver cancer