Bronchogenic Carcinoma types, stages, symptoms and diagnosis
Bronchogenic Carcinoma is a disease characterized by uncontrolled cell growth in tissues of the lung. If left untreated, this growth can spread beyond the lung in a process called metastasis into nearby tissue and, eventually, into other parts of the body. Most cancers that start in the lung, known as primary lung cancers, are carcinomas that derive from epithelial cells.
Bronchogenic Carcinoma
Bronchogenic carcinoma is the most common cause of cancer in men, and the 6th most frequent cancer in women worldwide. Bronchogenic carcinoma is the leading cause of cancer mortality worldwide in both men and women and accounts for approximately 20% of all cancer deaths.
Classification
Lung cancers are classified according to histological type. This classification has important implications for clinical management and prognosis of the disease. The vast majority of lung cancers are carcinomas-malignancies that arise from epithelial cells. Lung carcinomas are categorized by the size and appearance of the malignant cells seen by a histopathologist under a microscope. The two broad classes are non-small cell and small cell lung carcinoma.

Bronchogenic Carcinoma types
A. Non-small cell lung carcinoma (NSCLC)
There are three main sub-types:
Adenocarcinoma: Account for nearly 40% of lung cancers. This type of cancer usually originates in peripheral lung tissue. Common in Non-smokers. A subtype of adenocarcinoma, the bronchioloalveolar carcinoma, is more common in female never-smokers, and may have different responses to treatment.
Bronchioloalveolar carcinoma (Invasive adenocarcinoma): This neoplasm is a distinctive form of adenocarcinoma. The neoplasm arises from the epithelium of the terminal bronchiole or the alveolus. The neoplastic cells are columnar, lining alveoli or forming papillary growths which project into the alveolus. The neoplasm, almost always arising in the periphery, is solitary or forms multiple coalescing nodules. It is associated with excessive production of sputum (bronchorrhea).
Squamous cell lung carcinoma: Accounts for about 30% of lung cancers. They typically occur close to large airways. A hollow cavity and associated necrosis are commonly found at the center of the tumor.
Large cell lung carcinoma: Accounts for about 9% of lung cancers. These are so named because the cancer cells are large, with a lot of cytoplasm, large nuclei, and conspicuous nucleoli. They typically arise in the periphery.
B. Small cell lung carcinoma (SCLC)
- In.SCLC, the cells contain dense neurosecretory granules (vesicles containing neuroendocrine hormones), which give endocrine/paraneoplastic syndrome association.
- Most cases arise in the larger airways (primary and secondary bronchi).
- These cancers grow quickly and spread early in the course of the disease. 60- 70% have metastatic disease at presentation.
- This type of lung cancer is strongly associated with smoking and paraneoplastic manifestations.
C. Others
Including glandular tumors, carcinoid tumors, and undifferentiated carcinomas. These types are much less common than NSCLC and SCLC and together comprise only 5%-10% of lung cancers.
Bronchial carcinoids account for up to 5%-10% of lung cancers. These tumors are generally small (3-4 cm or less) when diagnosed and occur most commonly in persons under 40 years of age. Unrelated to cigarette smoking. carcinoid tumors can metastasize, and a small proportion of these tumors secrete hormone-like substances (serotonin). Carcinoids generally grow and spread more slowly than bronchogenic cancers, and many are detected early enough to be surgically removed.
Cancers of supporting lung tissue such as smooth muscle, blood vessels, or cells involved in the immune response can rarely occur in the lung.
D. Metastasis
The lung is a common place for metastasis of tumors from other parts of the body. Secondary cancers are classified by the site of origin, e.g., breast cancer that has spread to the lung is called metastatic breast cancer. Metastases often have a characteristic round appearance on chest radiographs.
Primary lung cancers themselves most commonly metastasize to the brain, bones, liver, and adrenal glands. Immunostaining of a biopsy is often helpful to determine the original source.
Clinical Presentation
- Asymptomatic (up to 50% of cases).
- Central airways: cough, hemoptysis.
- Peripheral airways: cough, pleuritic chest pain.
- Dyspnea.
- Pneumonia.
- Pleural effusion.
- Fixed inspiratory wheeze.
- Lymphadenopathy.
- Superior vena cava obstruction.
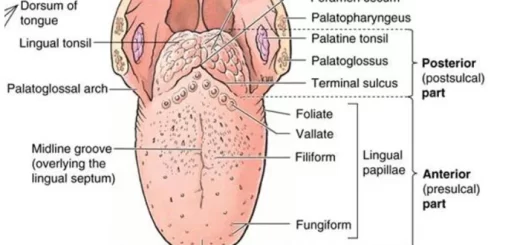
- Dysphagia (difficulty swallowing).
- Metastases (brain, liver, bone).
- Diaphragmatic paralysis.
Pancoast Tumor
- Horner’s syndrome.
- Hoarseness of voice.
Paraneoplastic syndromes
A. Endocrine
- SIADH causing hyponatremia.
- ACTH secretion (Cushing syndrome): small-cell subtype.
- PTHrp causing hypercalcemia: squamous cell carcinoma.
- Carcinoid syndrome.
- Gynecomastia.
B. Neurological
- Polyneuropathy Myelopathy.
- Cerebellar degeneration.
- Myasthenia: Eaton-Lambert syndrome.
C. Other
- Finger clubbing.
- Hypertrophic pulmonary osteoarthropathy (HPOA).
- Nephrotic syndrome.
- Polymyositis.
- Dermatomyositis.
- Eosinophilia.
- Acanthosis nigricans.
Causes
Cancer develops following genetic damage to DNA. This genetic damage affects the normal functions of the cell, including cell proliferation, programmed cell death (apoptosis), and DNA repair. As more damage accumulates, the risk of cancer increases.
- Smoking.
- Radon gas.
- Asbestos.
- Air pollution.
- Genetics.
Diagnosis
1. Chest radiograph: is one of the first investigative steps if a patient report symptoms that may suggest lung cancer. This may reveal an obvious mass, widening of the mediastinum (suggestive of spread to lymph nodes there), atelectasis (collapse), consolidation (pneumonia), diaphragmatic paralysis, bone erosion, pleural effusion, hyperinflation or may be normal.
2. CT scan (computerized tomography); is frequently the second step either to follow up on an abnormal chest X-ray finding, or to evaluate troublesome symptoms in those with a normal chest X-ray. CT scanning involves a series of X-rays that create a 3-dimensional view of the lungs. If the CT is abnormal, the diagnosis of lung cancer still needs confirmation through a sample of tissue by one of the procedures below.
3. MRI (magnetic resonance imaging): In some patients, MRI will be used to evaluate the possibility of lung cancer. This procedure uses magnetism and does not involve radiation. Certain individuals, such as those with metal implants (pacemakers, etc) should not have MRI scans.
4. PET scan: A PET scan uses radioactive material to create colorful 3-dimensional images of a region of the body. This type of scan differs from the others in that it defines tumors that are actively growing. As an addition to the other procedures, some researchers suggest that PET scanning may detect tumors earlier, even before they are visible anatomically through other studies.
5. Sputum cytology: After lung cancer is suspected based on imaging, a sample of tissue is required to confirm the diagnosis and determine the type of cancer. Sputum cytology is the easiest way to do this, but its use is limited to those tumors that extend into the airways. Sputum cytology is not always accurate and can miss some cancer cells.
6. Bronchoscopy: In a bronchoscopy, a lung specialist inserts a tube into the airways to visualize and take a sample of the tumor. This procedure is used when the tumor is found in the large airways and can be reached by the scope. Patients are given anesthesia during this procedure to minimize discomfort.
7. Needle Biopsy (fine needle aspiration): With this procedure, a hollow needle is inserted through the chest wall, usually guided by CT or U/S visualization, to take a sample of the tumor. This can be performed for tumors that cannot be reached by bronchoscopy (peripheral tumours).
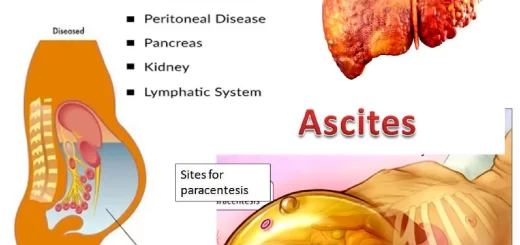
8. Thoracentesis: When lung cancer affects the periphery of the lungs, it can create a pleural effusion, With local anesthesia, a larger needle is inserted into the pleural space from which either a diagnostic amount of fluid (small amount to test for cancer cells) or a therapeutic amount of fluid (large amount to improve pain/shortness of breath) is removed.
9. Mediastinoscopy: This procedure is done in the operating room under general anesthesia. A scope is inserted just above the sternum (the breast bone) into the region between the lungs to take tissue samples from mediastinal lymph nodes.
10 . Tests to determine the spread of lung cancer (metastasis): Lung cancer most commonly spreads to the liver, the adrenal glands, the brain. and the bones. Common tests include:
- CT scan of the abdomen to check for spread to the liver or adrenal glands.
- CT scan of the brain– to look for metastases to the brain.
- Bone Scan-to test for bone involvement, especially the back, hips, and ribs.
11. Other tests during diagnosis: Additional non-diagnostic tests are frequently performed during the diagnosis of lung cancer as well. These can include:
- Pulmonary function tests – these test lung capacity and can determine how much the tumor is interfering with breathing, and sometimes, whether it is safe to perform surgery.
- Blood tests– certain blood tests can detect biochemical abnormalities caused by lung cancers and can also suggest the spread of the tumor (tumor markers).
The definitive diagnosis of lung cancer is based on histological examination of the suspicious tissue in the context of the clinical and radiological features.
You can subscribe to Science Online on YouTube from this link: Science Online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Pneumothorax causes, types, treatment, Who is at risk for pneumothorax?
Pleural disease symptoms and treatment, What is the most common pleural disease?
Bronchiectasis causes, Is a bronchiectasis serious?, What is the best medication for bronchiectasis?
Suppurative Lung Diseases, Stages of Lung Abscess, Does a lung abscess require surgery?
Tuberculosis symptoms, What causes TB disease? and Can TB be transmitted through saliva?
Inflammation of the lung parenchyma, What causes lung parenchyma?, Is lung parenchyma dangerous