Lose Weight with Intragastric Balloon, Bariatric Surgical, Sleeve gastrectomy benefits and risks
Intragastric balloon is a balloon manufactured from non-irritant material to be placed in the stomach by the aid of upper gastrointestinal endoscopy. After its placement in the stomach, it is inflated with methylene blue solution to a volume of 500-700 cc.
Intragastric balloon
An intragastric balloon is used for patients who are obese and have not been able to lose weight through diet and exercise alone, It is a non-surgical, temporary weight-loss device that is placed inside the stomach to help reduce food intake and promote a feeling of fullness.
The balloon is inserted into the stomach via an endoscopic procedure through the mouth, and it is filled with saline or gas to occupy space. Most balloons are left in place for 6 months, though some can remain up to 12 months. By taking up space in the stomach, the balloon helps patients feel full sooner and eat less.
Generally, it is recommended for individuals with a BMI of 30–40, or those with a lower BMI and obesity-related conditions. The balloon is deflated and removed using another endoscopic procedure. The intragastric balloon is non-surgical, reversible, and can result in 10–15% total body weight loss.

Sleeve gastrectomy vs. intragastric balloon
Intragastric balloon decreases the functional volume of the stomach to restrict food intake. It aims at a decrease of 25-30 kg of the patient’s body weight. It has the advantage of being a simple and short procedure. It is very useful as an adjuvant procedure before operating on super-obese patients to obtain some weight reduction, which helps in improving the outcome in such patients.
Its main disadvantage is that it must be removed after six months. So that most patients regain weight after its extraction. It is a temporary solution; it has side effects, including nausea, vomiting, and abdominal discomfort are common initially. The Risk of the Intragastric balloon is deflation, ulceration, or obstruction (though rare).
Bariatric Surgical
Bariatric surgery describes a group of operations performed primarily to reduce body weight (treat morbid obesity). This is typically achieved through inducing anatomical alteration to the GIT. These operations aim at:
- Reducing the morbidity and mortality associated with obesity.
- Improving metabolic and organ function.
- Decreasing food reservoir.
- speeding food passage through the GIT or shortening the journey through the bowel.
Indications
- BMI > 40
- BMI ≥ 35 + one or more co-morbidity (osteoarthritis, disc prolapse, DM2, hypertension, dyslipidemia, obstructive sleep apnea, etc).
Prerequisites for Having a Bariatric Operation
- Age: 18-65 y (patients outside this range are only operated upon in special conditions).
- Psychic stability & integrity.
- Normal eating behavior.
- Normal endocrine function.
- Ability & willingness to attend follow-up.
- Fitness for surgery.
- Failure of other measures of weight loss (diet & exercise).
- A multidisciplinary approach is MANDATORY. (The decision must include a committee from nutritionist, medical department, psychiatry, and surgery).
Procedure
Bariatric surgery requires special circumstances. One of the most important things is the operating table, as it must be able to carry the weight of the patient and secure him. We can move him back and through during the operation because during laparoscopic surgery, the patient is semi-sitting in front of the surgeon and is carried over a single joint of the table. It is very expensive. compared to the ordinary surgical table.
Bariatric operations are classified according to the mechanism of action into:
- Restrictive operations: This group of operations works mainly by limiting the food reservoir, which limits food intake. Rapid food passage occurs in some of these operations. This, when present, acts as a 2ry mechanism. (Lap. Band. Sleeve gastrectomy).
- Malabsorptive operations (Biliopancreatic diversion): Here, the main mechanism of action is to induce malabsorption through short-circuiting of the food passage via “bypassing” a variable length of the small intestine. All these operations also have a restrictive action added to them.
- Combination: In which we combine restrictive and malabsorptive operations to achieve the most benefits. Roux-en-Y gastric bypass. Single anastomosis gastric bypass.
Adjustable silastic gastric banding (lapBand)
An inflatable balloon within the band orifice can be adjusted via a reservoir under the skin. Average weight loss is 50% of the excess weight. It has the advantages of not changing the nature of the gastrointestinal tract. It’s reversible, as we can remove the end. The band can be implanted laparoscopily.
Its use has decreased markedly nowadays because of the hazards associated with it: around the band infections and penetration of the band in the stomach.
Procedure:
We do small incisions in which we insert our trocars through which the instruments enter the abdomen, we see and examine the gastrointestinal tract. Then we concentrate on the stomach, insert the band through one of the trocars and put it around the stomach, there is a lock which prevents the band from slipping.
There is a tube connected to an implantable subcutaneous reservoir, which we are going to implant by a special instrument. Then we inflate the balloon of the reservoir so the orifice decreases. The food is hindered by the band and gives the sensation of early satiety.
Sleeve gastrectomy
- Reduction in 75% of excess weight.
- As effective as RYGBP.
- Technically easy.
- Low mortality, 0.05% but is associated with some complications.
Procedure:
In this operation, we reduce the size of the stomach to a sleeve starting from the angle of his till about 6-8 cm from the pyloric ring by a series of stables. This is stabular device which is passing through the orifices of the laparoscopic equipment and then we start cutting this part of stomach.
We do small incisions in which we insert our trocars through which the instruments enter the abdomen, we explore the abdomen. The stomach is distended to 1500mm, and by the operation, it is reduced to 150mm so the amount of food needed to reach satiety is much less.
Advantages
Laparoscopic sleeve gastrectomy does not involve malabsorption, abnormal tracts, blind tracts, or the placement of a foreign body.
Complications of the operation
- Suture link leak.
- Bleeding.
- Dilatation of gastric remnants. It doesn’t happen till now. We do not see this dilatation but we can observe after 3 or 4 years, the patient regains his appetite again.
You can subscribe to Science Online on YouTube from this link: Science Online
Gastric neoplasms risks and types, Gastric Polyps, Gastric leiomyoma, and Gastric Cancer
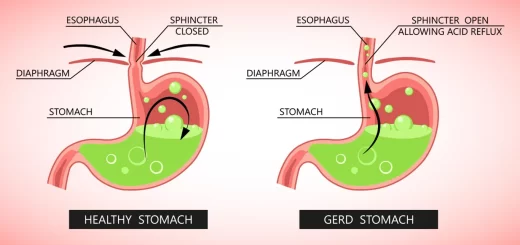
Gastroesophageal reflux disease (GERD) causes, treatment, and how to treat eosinophilic esophagitis?
Pharynx function, anatomy, location, muscles, structure, and Esophagus parts
Tongue function, anatomy and structure, Types of lingual papillae and Types of cells in taste bud
Mouth Cavity divisions, anatomy, function, muscles, Contents of Soft palate and Hard palate
Temporal and infratemporal fossae contents, Muscles of mastication and Otic ganglion
Stomach Cancer (Gastric Adenocarcinoma) Symptoms, Causes and Treatment