Neck mass symptoms, types, treatment, Malignant and Non-malignant neck lumps
The neck connects the head to the torso and contains vital structures from several systems. A neck mass refers to any abnormal lump or swelling in the neck. These can range from benign (non-cancerous) to malignant (cancerous) and may be caused by a variety of conditions.
Classification of Neck Mass
Neck masses can originate from: Skin, Endocrine organs, Upper aerodigestive Tract, Vessels, or Lymph Nodes. They are classified into: Congenital and Acquired.
- Inflammatory.
- Benign Neoplasm.
- Malignant Neoplasm.
Evaluation
Evaluation, which leads to the proper treatment and the best outcome, follows the following 4 steps:
- Appropriate initial assessment.
- Role and technique of FNAB.
- Appropriate use and interpretation of imaging
- Management: The importance of specialized multidisciplinary care if malignancy is suspected.

Neck mass
Appropriate Initial Assessment
A careful history and examination can often help make the correct diagnosis of a lump in the neck. The clinical signs of size, site, shape, consistency, fixation to skin or deep structures, pulsation, compressibility, transillumination, or the presence of a bruit remain as important as ever.
- Age.
- Location.
- Risk Factors.
- Symptoms.
- Head & Neck Exam.
- General physical exam.
Age
- Children (Pediatric): Inflammatory, congenital, and Malignant-
- Young Adult: Congenital, Inflammatory, and Malignant.
- Adult (>40): Malignant, Congenital, and Inflammatory.
Location
Common neck mass locations include the following:
- Angle of mandible: parotid swelling.
- Lateral neck: Enlarged lymph nodes (LNs) – Central compartment: Thyroid swelling.
Role of 80% of neck masses
Cases of neck masses: 80% are neoplastic, of which 80% are malignant, of which 80% are metastatic.
Risk Factors
- Tobacco.
- Alcohol.
- HPV (Human Papiloma Virus) and HN (Head and Neck cancer).
- Male predominance in Cancer.
- Younger patients.
- Fewer traditional risk factors.
- Sexual behavior as a risk factor for multiple sexual partners (>6), higher rates of oro-genital contact with multiple partners.
- Sun Exposure, Ex, farmer.
Symptoms of Head and Neck Primary
- Otalgia, unilateral.
- Hemoptysis.
- Nasal obstruction (snoring).
- Unilateral hearing loss.
- Dysphagia.
- Epistaxis.
- Hoarseness.
- Sore throat.
Symptoms of Lymphoma
- Fever.
- Night Sweats.
- Weight Loss.
Physical Exam: What do we need to document?
- Location of the mass in the neck.
- Presence/absence of a primary in the head and neck.
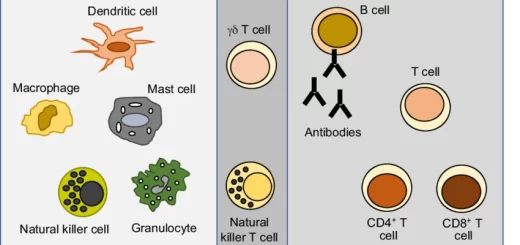
- Presence/absence of generalized lymphadenopathy.
Non-neck mass
- Transverse processes of cervical vertebrae.
- Carotid bulb.
- Inferior belly of the omohyoid.
Role and Technique of FNAR
- Needle size 25 gauge.
- 12-15 Passes should be performed.
- Immediate assessment of adequacy by the Pathologist is the rule.
Fine Needle Aspiration Biopsy
Diagnosis of Lymphadenopathy
- Sensitivity 85-97%.
- Specificity 98-100%.
- Nondiagnostic 8-16%.
- Open Biopsy 22-30%.
Role of Open Lymph Node Biopsy
- Excisional/Incisional Biopsy may be necessary:
- Sub classification of lymphoma.
- Facilitate the diagnosis of poorly differentiated carcinoma.
- Persistently nondiagnostic FNAB.
IV Management: The importance of specialized multidisciplinary care cannot be emphasized more, particularly if malignancy is suspected:
- Benign
- Malignant
Non-malignant neck lumps
- Bening.
- Inflammatory.
1. Cystic hygroma (Lymphangiomas)
- It is a congenital lesion usually present within the first year of life. (Posterior Triangle).
- Usually remain unchanged into adulthood.
- Soft, cystic, multilocular, partially compressible, and brilliantly transilluminant, and may present with pressure effects.
- CT or MRI may help define the extent of the neoplasm.
- Treatment of Lymphangiomas includes injection with picibanil or excision for easily accessible lesions or those affecting vital functions.
- If it affects vital function and structure.
- Injection is very hazardous.
2. Branchial cleft cysts
- Remnant of branchial cleft (2nd).
- Most commonly occur in the second or third decades.
- Pain +/- (severe throbbing pain) (not infected = mild aching pain).
- Usually presents as a smooth, fluctuant non non-tender (tender), non-transilluminant mass mobile forwards and downwards, underlying the anterior border of the sternomastoid muscle.
- Branchial fistula or sinus (infection).
- Primary treatment is with control of infection by antibiotics. followed by surgical excision.
3. Thyroglossal duct cyst
- This is a common congenital midline neck mass.
- Sometimes at the lateral edge.
- Pain and tenderness
- Can be moved transversally, but
- Elevates on the protrusion of the tongue.
- Treatment is with initial control of infection with antibiotics, followed by surgical excision including the mid-portion of the body of the hyoid bone (Sistrunk’s procedure).
- Occasionally, these lesions become infected and resolve, or persist following drainage as a thyroglossal fistula.
4. Lipoma
- Lipomas are the most common benign soft tissue neoplasm in the neck.
- They are poorly defined, soft masses usually after the fourth decade.
- They are usually asymptomatic, soft.
- FNAC or MRI Scan can confirm the diagnosis. MRI is the best.
- Surgery is indicated when the lump is increasing in size. cosmesis or when there is doubt about the accuracy of the diagnosis.
5. Sebaceous cysts
- These are common masses occurring often in older people, but can occur at any age.
- They are slow-growing, but sometimes fluctuant and painful when infected.
- Diagnosis is made clinically; the skin overlying the mass is adherent, and a punctum is often identified.
- Excisional biopsy confirms the diagnosis.
6. Cervical lymphadenopathy
Acute lymphadenitis
- tender swelling.
- Antibiotic trial, less acute inflammatory nodes generally regress in size over 2-6 weeks.
- If the lesion does not respond, the biopsy is warranted.
TB cervical lymphadenitis
- Upper and middle deep cervical LN.
- Onset: gradually.
- Pain: +/-
- Systemic symptoms are unusual in the young.
- Abscess (painful, increase size, and skin discoloration).
- Mass: indistinct, firm, matted, fluctuate!
- Temperature! (Cold abscess) (hot if see infection).
- Treatment with anti-TB (6- 9 months) Rifampicin Ethambutol INH Pyrazinamid.
7. Carotid body tumor
- Rare tumor of chemo receptors) (40-60 years).
- Slow-growing painless some time pulsating lump may be bilateral.
- Side-to-side movement (not along the carotid).
- Symptoms of transient cerebral ischemia!
- also known as Potato tumors (hard, non-tender).
- Palpation may induce a vasovagal attack.
- Biopsy is contraindicated: MRI (as its avascular mass).
- Angiography is the investigation of choice.
- Surgical removal is based on patient factors and presenting symptoms.
8. Pharyngeal pouch
- Diverticulum of the pharynx through the gap between the horizontal fibers of the cricopharyngeus muscle below and the lowermost oblique fibers of the inferior constrictor muscle above.
- History of froth and acid taste.
- Halitos is the regurgitation of food. There is no bile. or to it. (bad odor).
- Pressure on the swelling causes gurgling sounds and regurgitation.
- Treatment: cricopharyngeal myotomy.
9. Ludwig’s angina
- Rare but serious connective tissue infection of the floor of the mouth.
- Mostly due to dental infections.
- Signs of inflammation are present.
- Treatment: drainage of pus + antibiotic to cover aerobes with anaerobes.
10. Thyroid masses
- Thyroid neoplasms are a common cause of anterior compartment neck masses in age groups, with a female predominance, and are mostly benign.
- Fine needle aspiration of thyroid masses has become the standard of care, and ultrasound may show whether the mass is cystic.
- Unsatisfactory aspirates should be repeated, and negative aspirates should be followed up with a repeat FNAC and examination in 3 months.
Characteristics of malignant neck lumps
1. Lymphomas
- Painless lump: non-tender, smooth, and discrete.
- Slow growing.
- Patient presented with malaise, weight loss pallor.
- Fever, rigor and Hepatosplenomegaly.
- Mediastinal mass (SVC syndrome).
- Abdomin pressure on IVC may cause bi lateral leg oedma.
- Other lymph nodes in the axilla, groin, and abdomen should be examined.
- Treatment: according to stage (radiosensitive).
2. Metastatic Lymph Nodes (commonest)
- Upper cervical lymph nodes (upper aero-digestive tract).
- Accessory chain of nodes in the posterior triangle (Nasopharyngeal malignancies).
- (Occult primary) The most common sites are the tonsil, base of tongue, nasopharynx, and the Pyriform sinus.
- Virchow’s LN (Troisier ‘s sign), abdominal and thoracic malignancies.
- Painless, non-tender, and hard masses.
- Work up: Search for the primary and deal with it.