What are urinary tract infections?, kidney problems, Urinary retention and Bladder stones
Urinary tract infections (UTIs) are the most common type of urinary complaint. They are caused by bacteria that enter the urinary tract and multiply. Symptoms of a UTI can include burning or pain with urination, frequent urination, blood in the urine, and strong-smelling urine.
What are urinary condition disorders?
Urinary incontinence is the involuntary loss of urine. There are different types of urinary incontinence, such as stress incontinence, urge incontinence, and mixed incontinence.
Urinary retention can be caused by a blockage in the urinary tract, nerve damage, or weak bladder muscles. Symptoms of urinary retention can include difficulty urinating, a feeling of fullness in the bladder, and overflow incontinence (leakage of urine).
Bladder stones can be caused by a variety of factors, including dehydration, infection, and a diet high in oxalate. Symptoms of bladder stones can include pain or burning with urination, blood in the urine, and frequent urination. Kidney stones can cause severe pain and other symptoms, such as blood in the urine, nausea, and vomiting.

Urinary tract infections
Tips for preventing urinary complaints
Drink plenty of fluids throughout the day. You should wipe from front to back after using the toilet. You have to empty your bladder when you urinate and don’t hold urine for long periods. You should strengthen your pelvic floor muscles with Kegel exercises. If you smoke, quit smoking. Maintain a healthy weight. Eat a healthy diet that is low in oxalate and other substances that can form stones.
Urinary complaints
I. General symptoms
a. Nausea, vomiting and colonic complaints:
- Usually in association with renal colic due to: Common innervation with vagus nerve, and Peritoneal irritation.
- Associated with pyonephrosis and severe UTI due to the release of toxins in the blood.
- Manifestation of uremia.
b. Anemia due to:
- Hematuria.
- Renal failure.
- Paraneoplastic syndrome associated with renal cell carcinoma.
c. Anorexia and weight loss associated with genitourinary malignancy.
d. Metastatic manifestations e.g.:
- Bone deposits with prostate cancer may cause spinal cord compression and hip fracture.
- Lung deposits with renal cancer may cause respiratory complaints and hemoptysis.
- Liver metastasis leads to Jaundice and malignant ascites.
II. Local urinary symptoms
a. Pain:
i. Renal pain which may be colicky pain, dull aching pain, or dragging pain. Renal pain must be differentiated from radicular pain secondary to neurological disease.
ii. Ureteric pain:
Usually, colicky pain that radiates to:
- The upper third of the ureter radiates….. to the epigastrium and suprapubic region.
- The middle third ureter radiates…….around the umbilicus.
- Lower third ureter radiates……… to the ipsilateral testis.
- Vesico-ureteric stone (intramural stone) radiates….. to the tip of the penis or vulva.
iii. Bladder pain:
- Sense of discomfort at the suprapubic region.
- Maybe associated with lower urinary irritative symptoms eg frequency, urgency, and burning micturition.
- Maybe associated with hematuria.
- Maybe associated with the inability to void.
iv. Prostatic pain:
- Sense of heaviness in the perineum
- Radiates…….. to anus, low back, suprapubic region, and scrotum.
- May be associated with dysuria.
- May be associated with painful ejaculation.
v. Primary testicular pain:
- Mostly dull aching pain (due to stretch of the capsule).
- Radiates….. to the groin (along the course of the spermatic cord).
- Causes: varicocele, hydrocele, testicular tumors, orchitis.
b. Mass:
i. Renal mass:
- Site: it occupies the lumbar region.
- The renal angle is dull and full.
- The mass moves with respiration.
- You can insinuate your hand below the costal margin.
- There is a band of resonance by percussion over the mass due to the presence of the colon.
- Bimanually felt.
- The direction of growth is downwards.
ii. Urinary bladder mass:
- Site: suprapubic region.
- Smooth outline by palpation.
- You cannot feel the lower margin of the bladder.
- Dull on percussion.
- Bimanual examination: Hard mass in cancer, and Boggy mass in urine retention associated with a strong desire to micturate.
- The mass disappears with bladder evacuation if it is due to urine retention.
c. Hematuria:
Definition: presence of red blood cells in urine. (RBCs > 3/HPF in urine analysis).
Etiology:
- Congenital anomalies: e.g. (polycystic kidneys.)
- Traumatic lesions: injuries to kidneys, ureters, bladder, and urethra.
- Inflammation: e.g. cystitis and pyelonephritis.
- Tumors of the urinary tract e.g. bladder carcinoma and renal cell carcinoma.
- Stones of the urinary tract.
- Reno-vascular lesions e.g. renal hemangioma and arterio-venous fistula.
- Systemic lesions e.g. hemophilia, leukemia.
Degrees of hematuria
- Microscopic hematuria: normal coloration of urine.
- Gross hematuria:
- Mild hematuria: cloudy coloration of the urine (like tea).
- Massive hematuria: Dark red coloration of urine.
- Hematuria with blood clots) (May cause urine retention and the clots must be evacuated).
The degree of hematuria does not correlate with the severity of the cause. A small tumor can cause severe hematuria with clots, while an advanced tumor can cause microscopic hematuria. Minor injury to the urinary tract can cause severe bleeding while major injury may present with just cloudy urine. Large renal stones can cause microscopic hematuria while small ureteric stones can cause massive hematuria.
Hematuria Associated with other symptoms
- Hematuria + severe dysuria and frequency of short duration, especially in females is suggestive of acute cystitis.
- Hematuria + Obstructive urinary symptoms of long duration in elderly man is suggestive of BHP or prostatic carcinoma.
- Hematuria + an attack of renal colic is suggestive of a stone in the urinary tract.
- Hematuria + fracture of pelvic bones following a car accident is suggestive of bladder or urethral injury.
- Hematuria + fever and loin pain is suggestive of acute pyelonephritis)
- Asymptomatic hematuria: Malignant lesion in the urinary tract (commonest cause), and Benign lesion e g. reno-vascular lesions or silent renal stones.
Differential diagnosis: red coloration of urine because of drug intake e.g rifampicin or food intake e.g: beetroot
Relation to micturition
- Initial hematuria: urethral origin as in urethritis or urethral tumors
- Terminal hematuria: bladder in origin as in bladder tumors.
- Total hematuria: originates from kidneys, ureters or bladder.
d. Urethral discharge:
- Purulent discharge: A greenish or yellowish stain in a male’s underwear is noticed. It is caused by venereal diseases; e.g. Gonorrhea or Chlamydia infection.
- Prostatorrhea: A colorless viscid odorless discharge emerging from the urethral meatus. It is caused by hypersecretion from the para-urethral glands in young adults who are both sexually active and sexually abstinent, it is not a disease.
e. Lower urinary tract symptoms (LUTS):
- Irritative symptoms.
- Obstructive symptoms.
Irritative symptoms
Irritation of the sensory autonomic nerves underneath the bladder mucosa the trigone. Irritative symptoms include:
- Urgency: an intense desire to micturition. In severe cases, it may progress to urge incontinence
- Frequency: increase in the number of the act of micturition. The normal number of voids per day is 3 to 5 times).
a. Diurnal frequency: only occurs during daytime may be due to:
- Bladder stone.
- Diuretics and antihypertensives.
- Increased fluid intake and increased coffee intake.
- Psychic stress or anxiety.
b. Nocturnal frequency: The normal number of voids at night ranges from 0- I times. At night voiding may increase due to:
- Prostatic enlargement.
- Early symptom of congestive heart failure.
- Edema of the lower limbs.
c. Both diurnal and nocturnal frequency due to:
- Prostatic enlargement (late stages).
- Cystitis.
- Chronic renal failure.
- Diabetes mellitus.
- Contracted bladder due to Bilharzias, TB, and irradiation.
3. Incontinence: Involuntary passage of urine per urethra.
Types:
- Stress incontinence.
- Urge incontinence.
- Overflow incontinence.
- Mixed incontinence.
4. Dysuria: painful difficult micturition.
5. Strangury: painful intense discomfort with frequent voiding of small amounts of urine.
II. Obstructive urinary symptoms:
- Hesitancy: delay in the start of the act of micturition.
- Straining: increase intra-abdominal pressure to increase the intra-vesical pressure to overcome the urethral resistance.
- Decrease in the caliber and force of the urine stream.
- Intermittent and bifid stream.
- Sense of incomplete bladder evacuation.
- Retention of urine which may be acute, chronic, or acute on top of chronic.
f. Disturbance in the urine content:
- Hematuria.
- Pyuria: the presence of pus cells in urine. D.D chyluria.
- Crystalluria: the presence of crystals in the urine mainly urates and phosphates.
- Necroturial presence of necrotic tissue with urine is mainly associated with bladder carcinoma (squamous type).
- Pneumaturia: the presence of air with urine. Maybe due to: Uro-intestinal fistula, Gas producing organisms, and Following genitourinary endoscopic management.
g. Disturbance in the urine volume:
- Oliguria: urine output less than 500 ml per day in adults.
- Anuria: absence of urine output.
- Polyuria: excessive passage of large volumes of urine more than 2 liters per day.
h. Abnormalities in the external genitalia:
- Meatal: hypospadias, epispadias, presence of fibrous nodules, lichen sclerosis.
- Penis: curvature or short penis.
- Testis: undescended testis, testicular torsion, hydrocele, heamatocele.
- Spermatic cord: varicose veins, hernia, spermatocele.
- Hematospermia: the presence of blood with semen.
Physical examination
Kidney Swelling (e.g. hydronephrosis, tumor)
- Inspection: Visible mass in the lumbar region if hugely enlarged especially in a slim patient.
- Palpation: Fullness of the renal angle (the renal angle is normally empty on palpation). It is bimanually felt as it is a retroperitoneal organ.
- Percussion: The renal angle occupied by the kidney swelling is always dull on percussion (the renal angle is normally occupied by the colonic flexure.
Bladder Swelling
A full bladder, especially in advanced chronic retention, is felt as a midline abdomino-pelvic swelling with a smooth upper surface. It is dull on percussion.
Digital Rectal Examination (DRE)
1. Inspection: presence of piles, and sinuses.
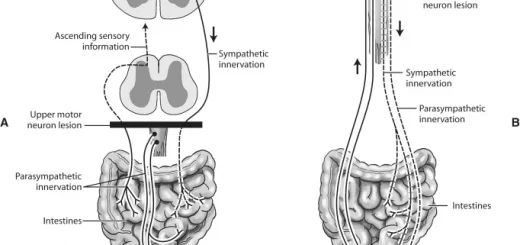
2. Anal sphincter: reduced tone of the anal sphincter with absent bulbo-cavernous reflex is suggestive of the neuropathic bladder (S2 – S4 supply both the bladder and anal canal).
3. Prostate:
a. Normal prostate: the size of a normal prostate is like walnut. It is easily felt with the front of the examining index finger.
b. Abnormal prostate:
- BPH: the size of the prostate is enlarged, rubbery in consistency, smooth surface, preserved median sulcus, and mobile overlying rectal mucosa.
- Prostate cancer: Nodular hard prostate, irregular surface, los median sulcus, and fixed overlying rectal mucosa.
- The prostatic abscess felt as tender boggy cystic lesion.
4. Bladder: the bladder base is normally felt by DRE.
Examination of the External Genitalia
- Penis: size, curvature, meatal stenosis, venereal warts, hypospadias, epispadias, abnormal nodules.
- Urethra: urethral discharge, urethral stone, meatal disease e.g. lichen sclerosis (whitish discoloration).
Examination of the Scrotal Contents
- Testis: hydrocele, tumors, absent testis, atrophied testis due to mumps orchitis, torsion.
- Epididymis: severely swollen and tender in acute epididymitis: indurated and nodular in T.B. epididymitis.
- Spermatic Cord: soft swelling (hernia, hydrocele), beading vas (T.B.). varicocele:
• Iry varicocele
- Grade 1: the smallest type, this is not visible but the physician can feel it if they use the Valsalva maneuver.
- Grade 2: this is not visible, but it can be felt without the Valsalva maneuver.
- Grade 3: the varicocele is visible.
• 2ry varicocele: 2ry to left renal cell carcinoma and malignant occlusion of the left renal vein. It does not evacuate while in the supine position.
You can subscribe to Science Online on YouTube from this link: Science Online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Functions of Kidneys, Role of Kidney in glucose homeostasis, Lipid & protein metabolism
Histological structure of kidneys, Uriniferous tubules and Types of nephrons
Urine formation, Factors affecting Glomerular filtration rate, Tubular reabsorption and secretion
Urinary passages function, structure of Ureter, Urinary bladder & Uvulae vesicae
Urinary system structure, function, anatomy, organs, Blood supply and Importance of renal fascia
Urinary bladder structure, function, Control of micturition by Brain & Voluntary micturition