Surgical Jaundice causes, symptoms, types, diagnosis and treatment
Surgical jaundice refers to obstructive jaundice that is caused by a mechanical blockage of the bile ducts, preventing bile from draining from the liver into the intestines. This type of jaundice often requires surgical intervention to remove the obstruction.
Definition of jaundice (Icterus)
Jaundice (icterus): yellowish staining of the skin, sclera and mucous membranes by deposition of bilirubin in these tissues. Jaundice indicates excessive levels of conjugated or unconjugated bilirubin in the blood and is clinically apparent when the bilirubin level exceeds 2mg/dl (Normal = 0.2-1 mg/dL).
Physiology/Biochemistry of Bilirubin production and transport:
- Composition of bile: bile salts, water, cholesterol, electrolytes, and bilirubin.
- Sources of bilirubin: 80% derived from heme of hemoglobin from senescent RBCs destroyed in the reticulo-endothelium of the bone marrow, spleen, and liver.
- 10-20% of the bilirubin comes from other sources.

Surgical Jaundice
Type of Jaundice
Jaundice is classified based on where the problem occurs in the metabolism or flow of bilirubin. The three main types of jaundice are:
1. Pre-Hepatic (Hemolytic) Jaundice
- Cause: Increased breakdown of red blood cells (hemolysis), leading to excess unconjugated bilirubin.
- Common Causes: Hemolytic anemia, Sickle cell disease, Thalassemia, Malaria, and Hereditary spherocytosis.
- Features: Elevated unconjugated (indirect) bilirubin, Normal liver function tests, and No bilirubin in urine (unconjugated bilirubin is not water-soluble).
2. Hepatic (Hepatocellular) Jaundice
- Cause: Liver cell damage impairs the liver‘s ability to process or excrete bilirubin.
- Common Causes: Hepatitis (viral, alcoholic, autoimmune), Cirrhosis, Liver cancer, Drug-induced liver injury.
- Features: Mixed increase of conjugated and unconjugated bilirubin, Elevated ALT and AST (liver enzymes), and Dark urine and possibly pale stools.
3. Post-Hepatic (Obstructive or Surgical) Jaundice
- Cause: Obstruction of bile flow after conjugation in the liver.
- Common Causes: Gallstones in the bile duct (choledocholithiasis), Pancreatic head carcinoma, Cholangiocarcinoma (bile duct cancer), Strictures or post-surgical bile duct injury.
- Features: Elevated conjugated (direct) bilirubin, Elevated alkaline phosphatase and GGT, Dark urine, pale stools, and itching (pruritus).
Causes of Surgical Jaundice
- Gallstones (choledocholithiasis) – stones blocking the common bile duct.
- Tumors: Pancreatic head cancer, Cholangiocarcinoma (bile duct cancer), and Ampullary carcinoma.
- Strictures – narrowing of the bile ducts due to inflammation, surgery, or injury.
- Parasites, such as liver flukes in endemic areas.
- Post-surgical injuries – bile duct injury after gallbladder removal (cholecystectomy).
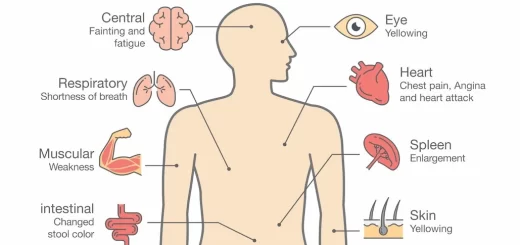
Symptoms of Surgical Jaundice
- Yellowing of the skin and eyes (jaundice).
- Dark urine.
- Pale stools.
- Itching (pruritus).
- Abdominal pain (especially in gallstone-related cases).
- Weight loss and anorexia (common in malignancies).
Diagnosis of Surgical Jaundice
Blood tests: Elevated bilirubin, alkaline phosphatase, GGT, and liver enzymes.
Imaging:
- Ultrasound: First-line for bile duct dilation or gallstones.
- CT scan or MRI/MRCP: Better for tumors or detailed duct imaging.
- ERCP (Endoscopic Retrograde Cholangiopancreatography): For diagnosis and possible treatment.
- Liver biopsy (rarely): To rule out hepatocellular disease if the diagnosis is unclear.
Treatment of Surgical Jaundice
Relieve obstruction:
- ERCP with stone extraction or stenting.
- Surgery – e.g., bile duct exploration or tumor resection.
- Percutaneous drainage (in some cases).
Treat the underlying cause, such as cholecystectomy for gallstones or chemotherapy for malignancy.
Surgically correctable jaundice
Surgical jaundice: any jaundice correctable by surgical intervention.
Types of surgically correctable jaundice: refers to a broader spectrum of diseases where surgery can relieve jaundice.
- Pre-hepatic (hemolytic) jaundice: Hereditary spherocytosis (HS): Inherited primarily in an autosomal dominant fashion, the Underlying abnormality is an inherited dysfunction or deficiency in one of the red cell membrane proteins, which results in destabilization of the membrane. This destabilization results in a lack of deformality (Normal RBCs are deformable), which sequestration and destruction of spherocytic red cells in the spleen, resulting in hemolytic anemia. Splenectomy is curative and serves as the sole mode of therapy.
- Hepatic jaundice: End-stage liver disease: requiring liver transplantation.
- Post-hepatic (Obstructive) jaundice:
Causes of obstructive jaundice:
Congenital
- Biliary atresia.
- Cystic Fibrosis Disease.
- Choledochal cysts.
Acquired
Gallstone disease. (Calcular O.J.):
- Choledocholithiasis: Primary: Formed inside the CBD (Less common), and Secondary: Migrating from the GB (more common).
- Mirizzi Syndrome.
Tumours (Malignant OJ):
- A. Primary: gall bladder, bile ducts (cholangiocarcinoma), head of pancreas, ampulla of Vater, and Periampullary region.
- B. Metastatic: deposited in the lymph nodes at the porta hepatis. Primaries of these metastatic deposits may be located in the lower esophagus, stomach, breast, and even the liver.
Trauma:
- latrogenic, e.g., during cholecystectomy, liver resections etc..
- Others e.g., stab, gunshot etc.
Strictures:
- Benign.
- Malignant.
- Primary sclerosing cholangitis.
Parasitic infections: Ascaris and Fasciola.
Clinical Features of Obstructive Jaundice
- Jaundice due to hyperbilirubinemia..
- dark urine (liquorice colored): because some conjugated bilirubin reaches kidneys.
- pale stools: because less bilirubin reaches the intestine.
- generalized pruritus: Due to High levels of circulating bile salts.
- Absence of bile salts can produce malabsorption, leading to steatorrhea and deficiencies of fat-soluble vitamins (particularly A, K, and D); vitamin K deficiency can reduce prothrombin levels and cause coagulopathy. A good history, physical examination, and diagnostic tests are the requisites for the evaluation of the jaundiced patient.
Investigations of obstructive jaundice
1. Biochemistry/Hematology
- Elevated serum bilirubin level with preponderance of conjugated fraction is the rule.
- The serum gamma-glutamyl transpeptidase (GGT) level is also raised in cholestasis.
- The alkaline phosphatase may be elevated up to ten times normal.
- Elevated WBC may be present in cholangitis.
- Tumor markers like CA 19-9, CEA and CA-125 are usually elevated in pancreatic cancers, cholangiocarcinoma, and peri-ampullary cancers, but they are nonspecific and may be elevated in other benign diseases of the hepatobiliary tree.
2. Imaging:
The goals of imaging are:
- to confirm the presence of an extrahepatic obstruction (i.e., to verify that the jaundice is indeed post-hepatic rather than hepatic).
- to determine the level of the obstruction.
- to identify the specific cause of the obstruction.
- to provide complementary information relating to the underlying diagnosis eg, staging information in cases of malignancy.
include:
1. Ultrasonography: The most important initial tool of investigation as it can provide sure evidence of biliary tree obstruction, namely intrahepatic bile duct dilatation.
In addition, it can provide data regarding:
- The size of the extrahepatic biliary tree.
- The level of the obstruction,
- May identify the cause and give other information related to the disease (e.g. gallbladder stones, hepatic metastases, hepatic parenchymal change).
2. Computed tomography (CT) of the abdomen is useful for:
- Staging of pancreatic and biliary malignancies.
- It provides excellent visualization tumor and its relation to surrounding structures.
- It provides excellent visualization of the liver and lymphadenopathies.
3. Endoscopic ultrasound (EUS) is useful for:
- Detection and staging of ampullary tumors.
- evaluation of benign and malignant bile-duct strictures, and finally, in evaluating relationships to vascular structures.
- Endoscopic ultrasound enables the aspiration of cysts and the biopsy of solid lesions.
4. Direct visualization of the biliary tree:
- Endoscopic retrograde cholangiopancreatography (ERCP)
- Percutaneous transhepatic cholangiography (PTC): provides direct visualization of the level of obstruction, However, both are invasive techniques and may be associated with complications such as cholangitis, biliary leakage, pancreatitis, and bleeding.
- Magnetic resonance cholangiopancreatography (MRCP): a noninvasive technique for visualization of the biliary and pancreatic ductal symptoms.
Diagnostic approach
- Question 1: Is jaundice obstructive?, If there are pale stools, dark urine, and pruritus, it’s obstructive jaundice.
- Question 2: What is the cause of the obstruction?, Malignant or Calcular. It’s known from the history of the patient.
- Question 3: What is the level of the obstruction? From radiology, we initially use US to demonstrate the dilatation in the biliary tree. If we suspect malignancy, the next step will be the CT. In other situations, we perform ERCP, PCT, or MRCP.
- Question 4: If the cause is malignant, what is the extent of the disease (staging)? From CT.
- Question 5: If it is malignant, is it respectable? From CT.
Treatment of obstructive jaundice: Treatment of the cause
You can subscribe to Science Online on YouTube from this link: Science Online
Gastric neoplasms risks and types, Gastric Polyps, Gastric leiomyoma, and Gastric Cancer
Gastroesophageal reflux disease (GERD) causes, treatment, and how to treat eosinophilic esophagitis?
Pharynx function, anatomy, location, muscles, structure, and Esophagus parts
Tongue function, anatomy and structure, Types of lingual papillae and Types of cells in taste bud
Mouth Cavity divisions, anatomy, function, muscles, Contents of Soft palate and Hard palate
Temporal and infratemporal fossae contents, Muscles of mastication and Otic ganglion
Stomach Cancer (Gastric Adenocarcinoma) Symptoms, Causes and Treatment