Pathology of gastric tumors, Gastric carcinoma classification and Treatment
Gastric tumors refer to abnormal growths in the stomach, and they can be either benign (non-cancerous) or malignant (cancerous). Types of Gastric Tumors are Benign Gastric Tumors and Malignant Gastric Tumors (Gastric Cancer).
Pathology of gastric tumors
The gastric cancer may arise in:
- The antrum (50%).
- The gastric body (30%).
- The fundus or the oesophago-gastric junction (20%).
Site of Stomach Cancer
- Antrum/lower 3rd: most predominant (40%).
- In the last decades, proximal cancers (cardia a GE junction) have risen from 10% to 30% of gastric cancers. This is because distal tumors are affected by altering the risk factors.
- There are also ↑ in tumors in the cardia region associated with gastro-esophageal reflux.
- Multicentric in 20% of cases.
Growth appearance:
- Polypoid.
- Fungating.
- Ulcerative.
- Scirrhous.
Ulcerated carcinoma (25%):
Deep penetrated ulcer with shallow edges.
Usually, through all layers of the stomach.
Polypoid carcinoma (25%):
- Intraluminal tumors, large in size.
- Late metastasis.
Superficial spreading carcinoma (15%):
- Confinement to mucosa and sub-mucosa.
- Metastasis 30% at time of diagnosis.
Linitis plastica (10%):
- A variety of superficial spreading carcinoma but involves all layers of the stomach.
- Early spread with poor prognosis.
Advanced carcinoma (35%):
- Partly within and outside the stomach.
- Represents the advanced stage of most of the four mentioned carcinomas.
Histology-Lauren Classification:
- Intestinal 54%.
- Diffuse 32%.
- Unclassified 15%.
There are two major types of gastric adenocarcinoma, including the following:
- Intestinal.
- Diffuse.
Intestinal adenocarcinomas are well differentiated, and the cells tend to arrange themselves in tubular or glandular structures. The terms tubular, papillary, and mucinous are assigned to the various types of intestinal adenocarcinomas. Rarely, adenosquamous cancers can occur.
Diffuse adenocarcinomas are undifferentiated or poorly differentiated, and they lack gland formation. Clinically, diffuse adenocarcinomas can give rise to infiltration of the gastric wall (i.e. linitis plastica)
Some tumors can have mixed features of intestinal and diffuse types.

Gastric tumors
Histologic type
- Papillary.
- Tubular
- Mucinous.
- Signet ring.
Microscopy
- Intestinal type (forms gland-like cancers of colon and oesophagus).
- Diffuse type-dissociated tumour cells often containing a mucinous “blob”-signet ring cells.
Gastric carcinoma classification
Depth of invasion
- Early gastric Cancer: confined to mucosa and submucosa, regardless of lymph nodes status.
- Advanced gastric Cancer: a tumor that has involved the muscularis propria.
Macroscopic growth pattern – Ming classification
- Expanding.
- Infiltrative – linitis plastica.
Histologic subtype
- Intestinal or well-differentiated.
- Diffuse or poorly differentiated; signet ring cell.
Staging of gastric cancer
- TNM system.
- CT staging.
- PHNS staging system, Japanese staging (Peritoneal dissemination, Hepatic metastasis, LN involvement, Serosal invasion).
Spread of gastric carcinoma
- Local infiltration → through the stomach wall to the peritoneum, pancreas, colon, etc.
- Direct extension: To the omentum, transverse colon, and mesocolon, and left lobe of liver. Extension of antral tumors to the duodenum. Extension of upper third tumors to the esophagus.
- Lymphatic → to Intraabdominal (frequent) →To LNs along the greater & lesser curvature, then to the celiac LNs, to the splenic hilum & root of mesentery, to retro-peritoneal & hepato-duodenal LNs & then to para-aortic nodes and supraclavicular lymph nodes (Troisier sign).
- Blood → liver and peritoneal cavity (more frequent), lungs.
- Transcoelomic → across the peritoneal cavity, often involves the ovaries.
- (Krukenberg tumour), periumbilical region (Sister Mary Joseph node) or peritoneal cul-de-sac (Blummers shelf).
- Malignant ascites.
Clinical manifestations
1. Symptoms
- Stomach cancer is often either Asymptomatic or has Nonspecific symptoms in its early stages (Vague discomfort or indigestion).
- Recent dyspepsia in a patient > 50 years and receiving treatment as a benign ulcer for 6-12 months without investigations.
- Alarm symptoms such as anorexia, weight loss, dysphagia, anaemia (Fe deficiency type) or gastrointestinal haemorrhage (occult blood, hematemesis or melena) usually indicate advanced disease.
- Symptoms are often absent in early stages, and when present, are often ignored, missed, or mistaken for another disease process.
- Proximal tumors may present with dysphagia.
- Antral tumors may present with outlet obstruction (pyloric obstruction).
By the time symptoms occur:
- Weight loss and pallor.
- Decreased food intake.
- Abdominal pain (Epigastric pain that is constant and non-radiating).
- Nausea, vomiting, and bloating.
- Acute GI bleeding & Chronic GI bleeding.
- Dysphagia.
2. Signs:
- Paraneoplastic syndromes: Trousseau’s syndrome -> thrombophlebitis:
- acanthosis nigricans -> hyperpigmentation of axilla and groin; peripheral neuropathy)
Signs of distant metastasis:
- Palpable abdominal mass, hepatomegaly, ascites, and jaundice.
- Epigastric mass (25% of cases): It usually denotes incurability but not irresistibility.
- To the neck (Virchow node).
- To the pelvis (Blumer shelf).
- To the ovaries (Krunkenberg tumors).
- To the peritoneum (ascites).
- Left axillary node (Irish).
- Sister Joseph nodule. periumbilical node.
- Pleural effusion.
- Aspiration pneumonitis.
3. Complications:
- Vomiting (gastric outlet obstruction by a pyloric tumor).
- Dysphagia (due to a tumor in the cardia).
- Acute presentation: hematemesis and melena (in advanced cases).
- Perforation.
- Presentation with metastases.
Evaluation of gastric cancer
- History.
- Clinical Examination.
- Investigations.
The clinical features of gastric cancer may arise from local disease, its complications, or its metastases.
Investigations:
1. Laboratory Studies:
- CBC count: May be helpful to identify anemia, which may be caused by bleeding, liver dysfunction, or poor nutrition; approximately 30: 40 % of patients have anemia.
- Stool examination for occult blood.
- Electrolyte panels.
- Liver function tests.
- Tumor markers such as CEA and CA 19-9: Elevated CEA in 45-65% of cases; elevated CA 19-9 in about 20% of cases.
2. Imaging Studies:
- Double-contrast upper GI series and barium swallows: May be helpful when obstructive symptoms are present or when bulky proximal tumors prevent passage of the enddoscope to examine the stomach distal to an obstruction.
- CT scanning or MRI of the chest, abdomen, and pelvis: To assess the local disease process and evaluate potential areas of spread.
- Endoscoping ultrasonography (EUS): Staging tool for preoperative assessment of the tumor stage. To assess the depth of the tumor (T) & detect enlarged perigastric & celiac lymph nodes (LNs).
- Barium studies: False negative in as many as 50% of cases, Sensitivity as low as 14% in early cases, May be superior to EGD for linitis plastica.
EGD may be normal, while “leather-bottle” will be apparent on radiograph. Double contrast barium swallow has 90% accuracy and is cost-effective. No ability to distinguish between malignant and benign ulcers. Chest radiography: To evaluate for metastatic lesions.
3. UGI ENDOSCOPY (The gold standard):
- Esophagogastroduodenoscopy (EGD): with multiple biopsy and brush cytology.
- It allows taking biopsies.
- Safe (in experienced hands).
Indications:
- New onset of dyspepsia > 45 years.
- Dyspepsia with alarm symptoms (weight loss, anaemia, recurrent vomiting, bleeding).
- Dyspepsia & family history of gastric carcinoma.
Patients in Asian countries are frequently diagnosed with gastric cancer at an earlier stage than in non-Asian countries. In Japan and Korea, where the incidence of gastric cancer is much higher than in Western countries, screening for gastric cancer is routine. You may see an ulcer (25%), polypoid mass (25%), superficial spreading (10%), or infiltrative (linnitis plastrica) – difficult to detect. Accuracy 50-95%, it depends on gross appearance, size, location & No. of biopsies.
4. Biopsy:
Multiple mucosal biopsies, in 6 in number, should be taken.
5. Laparoscopy:
To assess the stage and the curability of the disease.
Staging workup:
Serologic markers
- CEA, CA-125, CA 19-9, and CA 72-4 may be elevated but have low sensitivity/specificity.
- None are diagnostic.
- Preoperative elevation in markers usually indicates a high risk of adverse outcome.
- No serologic finding should exclude surgical consideration.
M Staging
- Conventional imaging with EUS and CT has a wide range of accuracy for detecting metastatic disease (sensitivity 37-46%, specificity 63-80%).
- The addition of PET (positron emission tomography) has significantly improved detection rates (sensitivity 69-78%, specificity 82-88%), and which is particularly advantageous for identifying unsuspected metastatic disease, which is present in up to 30% of patients at presentation.
Laparoscopy – washings
Laparoscopy is established for direct visualisation of low volume peritoneal and hepatic metastases as well as assessing local spread for operability, particularly in gastric cancer (Staging Laparoscopy). Exclude occult metastatic disease involving the peritoneum/diaphragm. PET, if available, may improve the detection of occult metastatic disease in some cases.
Differential diagnosis:
- Gastric ulcer. From history, Cancer is not relieved by antacids, not periodic, and not relieved by eating or vomiting.
- Other gastric neoplasms eg. GIST or lymphoma.
- Gastritis.
- Gastric Polyps.
- Crohns disease.
Preoperative Staging:
- Abdominal/pelvic.
- CT scanning.
- Endoscopic ultrasound (EUS).
- Depth of the tumor.
- Enlarged perigastric/celiac lymph nodes.
- Laparoscopy.
Preoperative Workup:
- Laparoscopy detected metastatic disease in 23 to 37% of patients deemed eligible for curative resection by CT scan.
- Laparoscopy improves palliation in these patients by avoiding unnecessary laparotomy in about one-fourth of patients presumed to have local disease on CT scan.
Treatment:
Preoperative Care:
- Preoperative staging is important because we do not want to subject the patient to radical surgery that cannot help him.
- Improve nutrition if needed by parenteral or enteral feeding.
- Correct fluid and electrolyte & anemia if they are present.
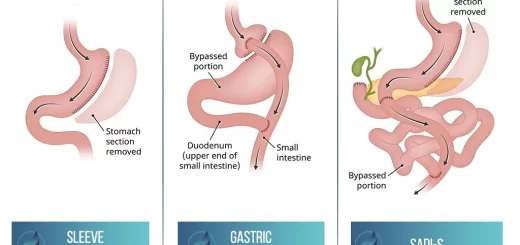
Treatment for Gastric Cancer
- Surgery: Endoscopic mucosal resection (EMR), Endoscopic submucosal dissection (ESD), Laparoscopic Surgery, and Open Surgery.
- Chemotherapy.
- Chemoradiotherapy.
- Target therapy.
Surgical resection remains the mainstay of treatment and is the only curative option. More recently, pre- and post-chemoradiation therapy has been scrutinized to see if there is any survival benefit.
The issue of the extent of resection appears to have been settled. As long as adequate tumor margins are achieved, subtotal gastrectomy has the same survival as total, with decreased morbidity.
1. Surgery
Endoscopic Mucosal Resection (EMR): is indicated for:
- TI Early lesions.
- Well differentiated.
- Small size (<3cm).
- No sub-mucosal involvement – chance of LN involvement – 0%.
- This approach involves the submucosal injection of fluid to elevate the lesion and facilitate complete mucosal resection under endoscopic guidance.
- Complications include – Bleeding and Perforation.
- Tumors invading the sub mucosa are at increased risk for metastasizing to lymph nodes and are not usually considered candidates for EMR.
Surgical Resection & Adequate Lymphadenectomy is the only curative treatment except for:
- Metastases.
- Co-morbidity.
Surgical removal of complete tumor + adjacent lymph nodes = only chance for cure; possible in < 30% of pts.
Basic surgical principles:
- 3 types: total, subtotal, palliative.
- Antral disease → Subtotal gastrectomy.
- Midway & Proximal → total gastrectomy.
The surgical approach in gastric cancer depends on the location, size, and locally invasive characteristics of the tumor.
Types of surgical intervention in gastric cancer include the following:
- Total Gastrectomy is required for negative margins.
- Esophago-Gastrectomy, for tumors of the cardia and gastroesophageal junction.
- Subtotal Gastrectomy for tumors of the distal stomach.
Objective
Removal of the tumor + uninvolved stomach margin (minimum 5 cm) and duodenum + regional LNs (corresponding to the location of the tumor) + adjacent organs (if involved).
Antral tumor: Distal gastrectomy + omentectomy + 3-4 cm duodenum + sub-pyloric LNs + reconstruction with GJ or gastro-duodenostomy.
Body tumor and extensive tumors: Total gastrectomy + splenectomy (debatable) + reconstruction (pouch or Roux-en-Y esophago-jejunostomy).
Routine splenectomy does not improve survival. Thus, splenectomy should not be performed unless there are adhesions with the tumor or infiltration of the spleen.
Cardia tumor: Esophago-gastrectomy (via 2 incisions)
Total (Radical) Gastrectomy and Oesophagojejunostomy Roux-en-y
- Remove the stomach + distal part of the esophagus + proximal part of the duodenum + greater & lesser omentum + LNs.
- Oesophagojejunostomy with Roux-en-Y.
Total Gastrectomy (TG) is indicated for:
- Diffuse involvement of the stomach.
- Large tumors are more than 5cm.
- Proximal tumors.
Prognosis:
- 5-year survival for TG- 10-15%.
- Inferior results due to large tumors & unfavorable proximal lesions.
- Laparoscopic approaches are being tried.
- Advantages of reduced pain, shorter hospitalization & improved quality of life.
- Long-term outcome to cancer recurrence awaits.
You can subscribe to Science Online on YouTube from this link: Science Online
Gastroesophageal reflux disease (GERD) causes, treatment, and how to treat eosinophilic esophagitis?
Pharynx function, anatomy, location, muscles, structure, and Esophagus parts
Tongue function, anatomy and structure, Types of lingual papillae and Types of cells in taste bud
Mouth Cavity divisions, anatomy, function, muscles, Contents of Soft palate and Hard palate
Temporal and infratemporal fossae contents, Muscles of mastication and Otic ganglion
Stomach parts, function, curvatures, orifices, peritoneal connections and Venous drainage of Stomach
Stomach Cancer (Gastric Adenocarcinoma) Symptoms, Causes and Treatment